SPECIAL FORMS OF ICD
SPECIAL FORMS OF ICD Hand Dermatitis Most cases of chronic ICD occur on the hands and are occupational. Often sensitization to allergens (such as nickel or chromate salts) occurs later, and then ACD is superimposed on ICD. A typical example is hand dermatitis in construction and cement workers. Cement is alkaline and corrosive, leading to chronic ICD (Fig. 2-4B); chromates in cement sensitize and lead to ACD (Allergic Contact Dermatitis, see below). In such cases, the eruption may spread beyond the hands and may even generalize. AIRBORNE ICD Characteristically on the face, neck, anterior chest, and arms. Most frequent causes are irritating dust and volatile chemicals (ammonia, solvents, formaldehyde, epoxy resins, cement, fiberglass, or sawdust from toxic woods). This has to be distinguished from airborne allergic contact dermatitis (Airborne Allergic Contact Dermatitis, p. 33) and photoallergic contact dermatitis (Section 10).
Pustular and Acneiform ICD ICD may target follicles and become pustular and papulopustular. Results from metals, mineral oils, greases, cutting fluids, and naphthalenes.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Diagnosis is by history and clinical examination (lesions, pattern, and site). Most important differential diagnosis is ACD (Table 2-3). On the palms and soles, palmoplantar psoriasis; in exposed sites, photoallergic contact dermatitis.
COURSE AND PROGNOSIS
Healing usually occurs within 2 weeks of removal of noxious stimuli; in more chronic cases, 6 weeks or longer. In the setting of occupational ICD, only one-third of individuals have complete remission and two-thirds
MANAGEMENT Prevention
• Avoid irritant or caustic chemical(s) by wearing protective clothing (i.e., goggles, shields, and gloves).
• If contact does occur, wash with water or weak neutralizing solution.
• Barrier creams.
• In occupational ICD that persists in spite of adherence to the preceding measures, a change of job may be necessary.
TREATMENT
Acute Identify and remove the etiologic agent. Apply wet dressings with Burow’s solution, changed every 2 to 3 hours. Larger vesicles may be drained. Topical class I–II glucocorticoid preparations. In severe cases, systemic glucocorticoids may be indicated. Prednisone taper over 2 to 3 weeks, starting at 1 mg/kg.
Subacute and Chronic Remove etiologic/ pathogenic agent. Potent topical glucocorticoids (betamethasone dipropionate or clobetasol propionate) and adequate lubrication. As healing occurs, continue with lubrication. The topical calcineurin inhibitors, pimecrolimus and tacrolimus, are usually not potent enough to sufficiently suppress the chronic inflammation on the hands. In chronic ICD of the hands, a “hardening effect” can be achieved in most cases with topical (soak or bath) Psoralen plus Ultraviolet A (PUVA) therapy (p. 63). SYSTEMIC TREATMENT Alitretinoin (approved in Europe and Canada) 0.5 mg/kg orally for up to 6 months. Observe contraindications to systemic retinoids.
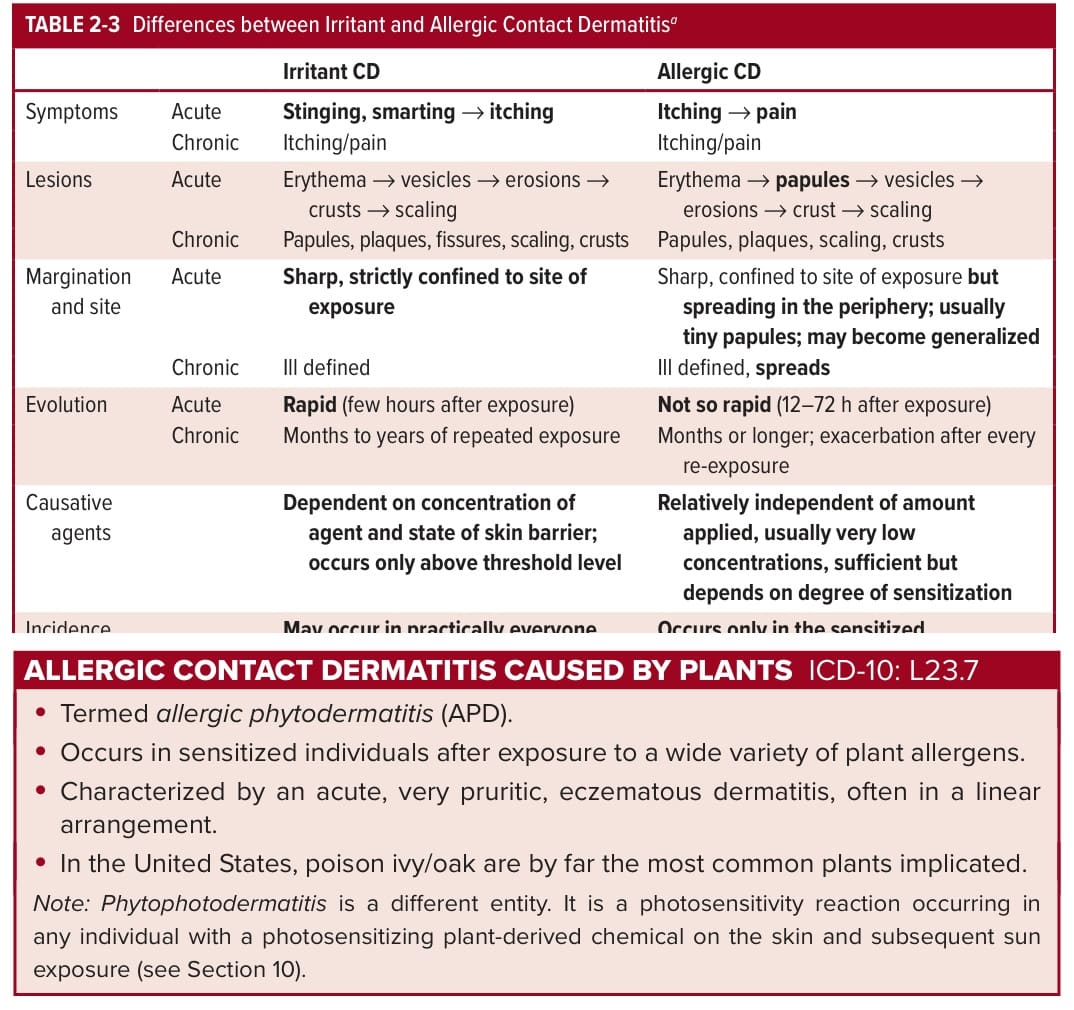
TABLE 2-3 Differences between Irritant and Allergic Contact Dermatitisa