ALLERGIC CONTACT DERMATITIS (ACD)
ALLERGIC CONTACT DERMATITIS (ACD) ICD-10: L24
• ACD is a systemic disease defined by hapten-specific T-cell–mediated inflammation.
• One of the most frequent, vexing, and costly skin problems.
• An eczematous (papules, vesicles, or pruritic) dermatitis.
• Caused by re-exposure to a substance to which the individual has been sensitized.
EPIDEMIOLOGY
FREQUENT Accounts for 7% of occupationally related illnesses in the United States, but data suggest that the actual incidence rate is 10 to 50 times greater than reported in the U.S. Bureau of Labor Statistics data. Nonoccupational ACD is estimated to be three times greater than occupational ACD. AGE OF ONSET All ages, but uncommon in young children and individuals older than 70 years. OCCUPATION One of the most important causes of disability in industry.
PATHOGENESIS
ACD is a classic, delayed, cell-mediated hypersensitivity reaction. Exposure to a strong sensitizer results in sensitization in a week or so, while exposure to a weak allergen may take months to years for sensitization. Sensitized T cells circulate in the blood and home to the skin wherever the specific allergen is presented. Thus, all skin is hypersensitive to the contact allergen.
ALLERGENS
Contact allergens are diverse and range from metal salts to antibiotics and dyes to plant products. Thus, allergens are found in jewelry, personal care products, topical medications, plants, house remedies, and chemicals the individual may come in contact with. The most common allergens in the United States are listed in Table 2-2.
CLINICAL MANIFESTATION
The eruption starts in a sensitized individual 48 hours or days after contact with the allergen; repeated exposures lead to a crescendo reaction, that is, the eruption worsens. The site of the eruption is confined to the site of exposure. SYMPTOMS Intense pruritus; in severe reactions, also stinging and pain. CONSTITUTIONAL SYMPTOMS “Acute illness” syndrome, including fever, but only in severe ACD (e.g., poison ivy, see below).
Skin Lesions
Acute Well-demarcated erythema and edema with superimposed closely spaced papules or nonumbilicated vesicles (Fig. 2-5); in severe
Nickel Metals in clothing, jewelry, catalyzing agents
Methylisothiazolinone Cosmetics, household products
Fragrance mix, 8%
Formaldehyde, 2% Preservative
Methylisothiazolinone/ methylchloroiso thiazolinone
Cosmetics, household products
Balsam of Peru Fragrance, flavoring agents
Neomycin Topical antibiotic
Bacitracin Topical antibiotic
Formaldehyde, 1% Preservative
Carba Rubber accelerator
Lanolin Creams, ointments
Source: Reproduced with permission from DeKoven JG, Warshaw EM, Zug KA, et al. North American Contact Dermatitis Group Patch Test Results: 2015–2016. Dermatitis. 2018;29(6):297–309.
reactions, bullae, confluent erosions exuding serum, and crusts. The same reaction can occur after several weeks at sites not exposed.
Subacute Plaques of mild erythema showing small, dry scales; sometimes associated with small, red, pointed, or rounded erythematous firm papules and scales (Figs. 2-6 and 2-7).
Chronic Plaques of lichenification (thickening of the epidermis with deepening of the skin lines in parallel or rhomboidal pattern), scaling with satellite, small, firm, rounded or flat-topped papules, excoriations, and pigmentation. ARRANGEMENT Initially, confined to the area of contact with the allergen (e.g., earlobe [earrings], dorsum of foot [shoes], wrist [watch or watchband], collar-like [necklace], and lips [lipstick]). Often linear, with artificial patterns, an “outside job.” Plant contact often results in linear lesions (e.g., Rhus dermatitis, see below). Initially confined to the site of contact, then later spreading beyond. DISTRIBUTION Extent Isolated, localized to one region (e.g., shoe dermatitis) or generalized (e.g., plant dermatitis).
COURSE
EVOLUTION OF ACD The duration of ACD varies, resolving in around 1 to 2 weeks, but
becomes worse as long as the allergen continues to come into contact with the skin.
Acute Erythema → papules → vesicles → erosions → crusts → scaling.
Note: In the acute forms of contact dermatitis, papules occur only in ACD, not in ICD (see Table 2-3).
Chronic Papules → scaling → lichenification → excoriations.
Irritant CD Allergic CD
Symptoms Acute Stinging, smarting → itching Itching → pain Chronic Itching/pain Itching/pain
Lesions Acute Erythema → vesicles → erosions → crusts → scaling Erythema → papules → vesicles → erosions → crust → scaling Chronic Papules, plaques, fissures, scaling, crusts Papules, plaques, scaling, crusts
Margination and site Acute Sharp, strictly confined to site of exposure Sharp, confined to site of exposure but spreading in the periphery; usually tiny papules; may become generalized Chronic Ill defined Ill defined, spreads
Evolution Acute Rapid (few hours after exposure) Not so rapid (12–72 h after exposure) Chronic Months to years of repeated exposure Months or longer; exacerbation after every re-exposure
Causative agents Dependent on concentration of agent and state of skin barrier; occurs only above threshold level
Relatively independent of amount applied, usually very low concentrations, sufficient but depends on degree of sensitization
Incidence May occur in practically everyone Occurs only in the sensitized
aDifferences are printed in bold.
Note: ACD is always confined to the site of exposure to the allergen. Margination is originally sharp, but it spreads in the periphery beyond the actual site of exposure. In the case of strong sensitization, it spreads to other parts of the body and generalization can occur. The main differences between toxic irritant and ACD are summarized in Table 2-3.
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY Acute Prototype of spongiotic dermatitis, with intercellular edema (spongiosis), lymphocytes and eosinophils in the epidermis, and monocyte and histiocyte infiltration in the dermis.
Chronic Also spongiosis plus acanthosis, elongation and broadening of papillae; hyperkeratosis; and a lymphocytic infiltrate. PATCH TESTS In ACD, sensitization is present on every part of the skin. Therefore,
application of the allergen to any area of normal skin provokes an eczematous reaction. A positive patch test shows erythema and papules, as well as possibly vesicles confined to the test site. Patch tests should be delayed until the dermatitis has subsided for at least 2 weeks and should be performed on a previously uninvolved site.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
By history and clinical findings, including evaluation of site and distribution. Histopathology may be helpful; verification of offending agent (allergen) by patch test. Exclude ICD (Table 2-3), atopic dermatitis (AD), seborrheic dermatitis (SD) (face), psoriasis (palms and soles), epidermal dermatophytosis (KOH), fixed drug eruption, and phytophotodermatitis.

FIGURE 2-5 • Acute allergic contact dermatitis on the lips caused by lipstick The patient was hypersensitive to eosin. Note bright erythema, microvesiculation. At close inspection, a papular component can be discerned. At this stage, there is still sharp margination.

FIGURE 2-6 • Allergic contact dermatitis of hands: chromates Confluent papules, vesicles, subacute erosions, and crusts on the dorsum of the left hand in a construction worker who was allergic to chromates.

FIGURE 2-7 • Allergic contact dermatitis resulting from nickel, subacute Note a mix of papular, vesicular, and crusted lesions and loss of sharp margination. The patient was a retired watchmaker who used a metal clasp on the dorsum of the left hand while repairing watches. He was known to be allergic to nickel.
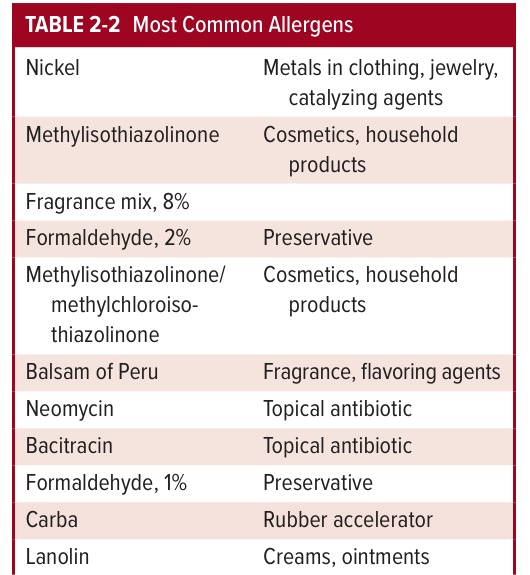
TABLE 2-2 Most Common Allergens
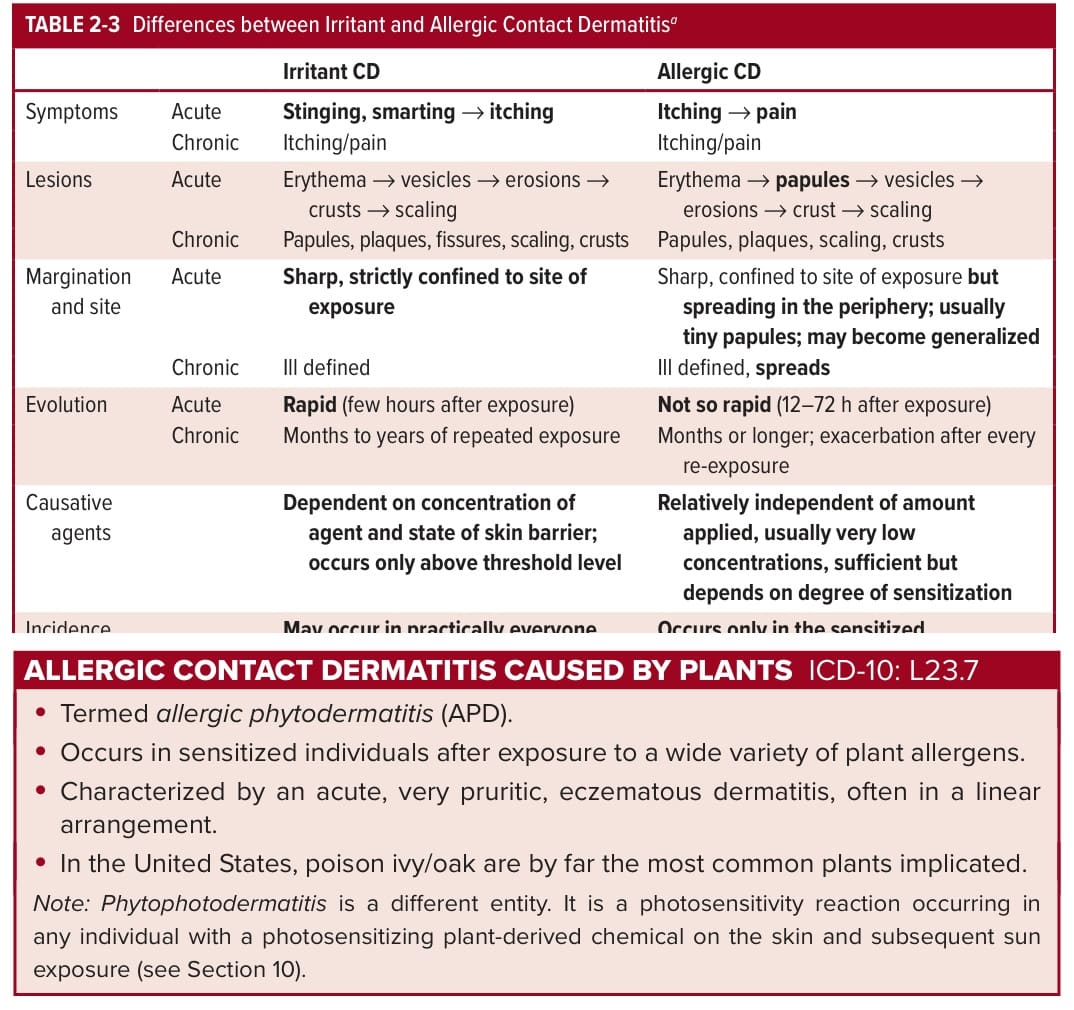
TABLE 2-3 Differences between Irritant and Allergic Contact Dermatitisa