AIRBORNE ACD
AIRBORNE ACD
• Contact with airborne allergens in exposed body sites, notably the face (Fig. 2-11) including the eyelids, “V” of the neck, arms, and legs.
• In contrast to airborne ICD, papular from the beginning, extremely itchy.
• Prolonged repetitive exposure leads to dry, lichenified ACD with erosions and crusting (Fig. 2-11).
• Caused by plant allergens, especially from compositae, natural resins, woods, and essential oils volatizing from aroma therapy.
MANAGEMENT OF ACD
TERMINATION OF EXPOSURE Identify and remove the etiologic agent. TOPICAL THERAPY Topical glucocorticoid ointments/gels (classes I–III). Larger vesicles may be drained, but tops should not be removed. Wet dressings with cloths soaked in Burow’s solution changed every 2 to 3 hours. Airborne ACD may require systemic treatment. Pimecrolimus and tacrolimus are effective in
ACD but to a lesser degree than glucocorticoids. SYSTEMIC THERAPY Glucocorticoids are indicated if severe and in airborne ACD. Prednisone beginning at 1 mg/kg, tapering over a 2- to 3-week period. In airborne ACD where complete avoidance of allergen may be impossible, immunosuppression with oral cyclosporine may become necessary.
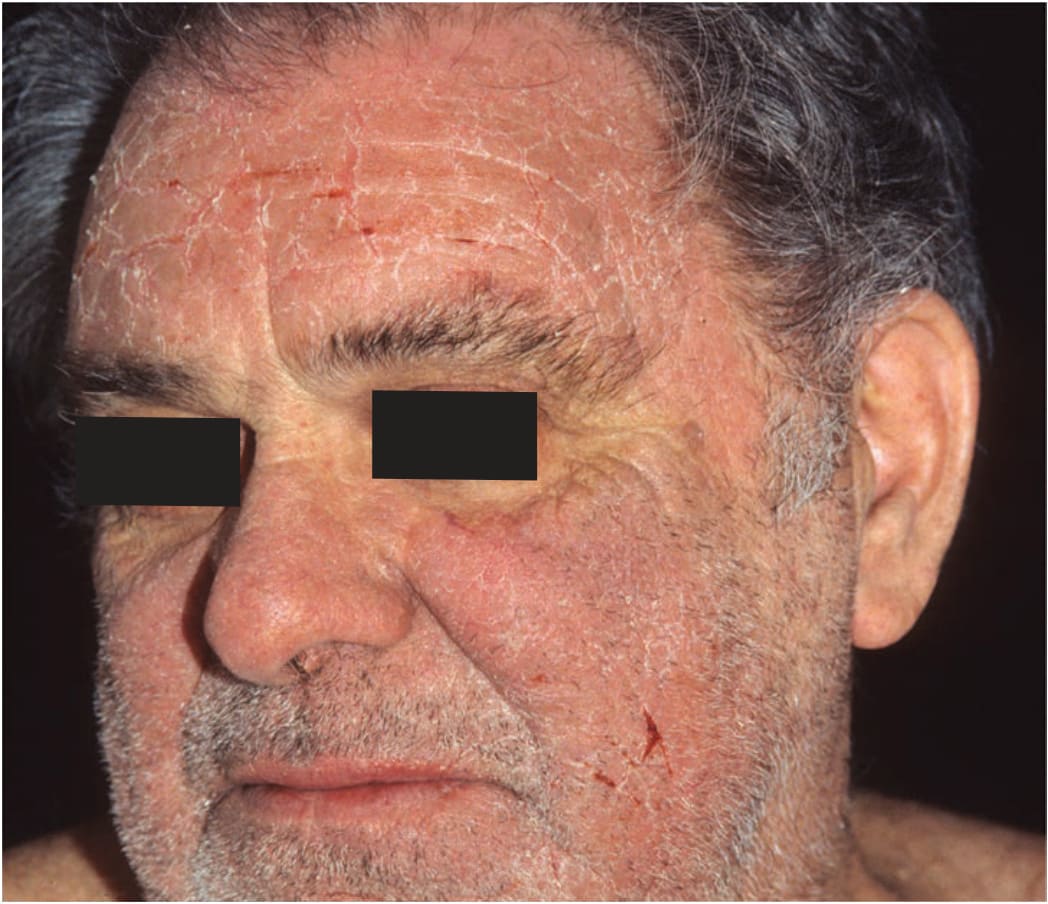
FIGURE 2-11 • Airborne allergic contact dermatitis of the face Extremely itchy, confluent, papular, erosive, and crusted/scaly lesions with lichenification on the forehead, nose, and cheeks following exposure to pinewood dust.