ATOPIC DERMATITIS
ATOPIC DERMATITIS ICD-10: L20
• An acute, subacute, or chronic relapsing skin disorder.
• Very common in infancy. Prevalence peak of 15% to 20% in early childhood.
• Characterized principally by dry skin and pruritus; consequent rubbing leads to increased inflammation and lichenification as well as to further itching and scratching: itch–scratch cycle.
• Diagnosis is based on clinical findings.
• Often associated with a personal or family history of AD, allergic rhinitis, and asthma; 35% of infants with AD develop asthma later in life.
• Associated with skin barrier dysfunction, IgE reactivity.
• Genetic basis influenced by environmental factors; alterations in immunologic responses in T cells, antigen processing, inflammatory cytokine release, allergen sensitivity, and infection.
Synonyms: IgE dermatitis, “eczema,” atopic eczema.
EPIDEMIOLOGY
AGE OF ONSET First 2 months of life and by the first years in 60% of patients; 30% by age 5, and only 10% between age 6 and 20 years. Rarely AD has an adult onset. GENDER Slightly more common in males than in females. PREVALENCE 7.3% of adults in the United Sates are affected by AD. GENETIC ASPECTS The inheritance pattern not yet ascertained. However, in one series, 60% of adults with AD had children with AD. The prevalence in children was higher (81%) when both parents had AD.
Skin Barrier Disruption Decrease in barrier function resulting from impaired filaggrin production, reduced ceramide levels, and increased transepidermal water loss; dehydration of skin. ELICITING FACTORS Inhalants Specific aeroallergens, especially dust mites and pollens.
Microbial Agents Exotoxins of Staphylococcus aureus acting as superantigens. Also, group A streptococcus, rarely fungus (candida).
Autoallergens IgE antibodies directed at human proteins. Release of these autoallergens from damaged tissue could trigger IgE or T-cell responses, suggesting maintenance of allergic inflammation.
Foods Infants and children, but not adults, have flares of AD with eggs, milk, peanuts, soybeans, fish, and wheat.
Other Exacerbating Factors
Season In temperate climates, AD usually improves in summer and flares in winter. Clothing Pruritus flares after taking off clothing. Wool is an important trigger; wool clothing or blankets directly in contact with skin (also wool clothing of parents, fur of pets, and carpets). Emotional Stress Results from the disease or is itself an exacerbating factor in flares of the disease.
PATHOGENESIS
Complex interaction of skin barrier, genetic, environmental, pharmacologic, and immunologic factors. Type I (IgE-mediated) hypersensitivity reaction as a result of the release of vasoactive substances from mast cells and basophils sensitized by the interaction of the antigen with IgE (reaginic or skin-sensitizing antibody). High-affinity IgE receptors on Langerhans cells may mediate the eczema-like reaction. Acute AD is associated with a predominance of interleukin (IL) 4 and IL-13 expression, and chronic inflammation in AD with increased IL-5, granulocyte-macrophage colony-stimulating factor, IL-12, and interferon-γ. Thus, skin inflammation in AD shows a biphasic pattern of T-cell activation.
CLINICAL MANIFESTATION
SKIN SYMPTOMS Patients have dry skin. Pruritus is the sine qua non of AD—“eczema is the itch that rashes.” The constant scratching leads
to a vicious cycle of itch → scratch → rash → itch → scratch. OTHER SYMPTOMS OF ATOPY Allergic rhinitis, obstruction of nasal passages, conjunctival and pharyngeal itching, and lacrimation; seasonal when associated with pollen. SKIN LESIONS Acute Poorly defined erythematous patches, papules, and plaques with or without scale. Edema with widespread involvement; skin appears “puffy” and edematous (Fig. 2-12). Erosions: moist, crusted. Linear or punctate, resulting from scratching. Secondarily infected sites: S. aureus. Oozing erosions (Fig. 2-12) and/or pustules (usually follicular). Skin is dry, cracked, and scaly (Figs. 2-12 and 2-13).
Chronic Lichenification (thickening of the skin with accentuation of skin markings) (Figs. 2-14 and 2-15B); follicular lichenification (especially in brown and black persons) (Figs. 2-14B and 2-15B). Fissures: painful, especially in flexures (Fig. 2-14A), often on the palms, fingers, and soles. Alopecia: lateral one-third of the eyebrows as a result of rubbing. Periorbital pigmentation, also as
a result of compulsive rubbing. Characteristic infraorbital fold below eyelids (Dennie– Morgan sign) (Adult Atopic Dermatitis, see Fig. 2-17).
Distribution Predilection for the flexures, front and sides of the neck, eyelids, forehead, face, wrists, and dorsa of the feet and hands (Fig. 2-16). Generalized in severe disease (Fig. 2-15A and B).
Special Features Related to Age
Infantile AD The lesions present as red skin, tiny vesicles on “puffy” surface. Scaling, exudation with wet crusts and cracks (fissures) (Figs. 2-12 and 2-13).
Childhood-Type AD The lesions are papular, lichenified plaques, erosions, crusts, especially on the antecubital and popliteal fossae (Fig. 2-14A and B), the neck and face; may be generalized.
Adult-Type AD There is a similar distribution, mostly flexural but also face and neck, with lichenification and excoriations being the most conspicuous symptoms (Figs. 2-15B and 2-17). May be generalized (Fig. 2-15B).
A B
A
B
Special Features Related to Ethnicity In African Americans and also in dark-brown skin, so-called follicular eczema is common, characterized by discrete follicular papules (Fig. 2-14B) involving hair follicles of the involved site.
Associated Findings
“WHITE” DERMATOGRAPHISM Stroking of involved skin will not lead to redness as in normal skin but to blanching; delayed blanch to cholinergic agents. Ichthyosis vulgaris and keratosis pilaris (see Section 4) occur in 10% of patients. Vernal conjunctivitis with papillary hypertrophy or cobblestoning of upper eyelid conjunctiva. Rare atopic keratoconjunctivitis is disabling and may result in corneal scarring. Keratoconus is rare. Cataracts occur in a very small percentage.
DIAGNOSIS
History in infancy, clinical findings.
DIFFERENTIAL DIAGNOSIS
SD, ICD, ACD, psoriasis, nummular eczema, dermatophytosis, or early stages of mycosis fungoides. Rarely, acrodermatitis enteropathica, glucagonoma syndrome, histidinemia, phenylketonuria; also, some immunologic disorders including Wiskott–Aldrich syndrome, X-linked agammaglobulinemia, hyper-IgE syndrome, and selective IgA deficiency; Langerhans cell histiocytosis.
LABORATORY EXAMINATIONS
BACTERIAL CULTURE Colonization with S. aureus is very common in the nares and in the involved skin; almost 90% of patients with severe AD are secondarily colonized/infected. Look out for methicillin-resistant S. aureus (MRSA). VIRAL CULTURE Rule out herpes simplex virus (HSV) infection in crusted lesions (eczema herpeticum; see Section 27). BLOOD STUDIES Increased IgE in serum, eosinophilia. HSV antigen detection for diagnosis of acute HSV infection. DERMATOPATHOLOGY Various degrees of acanthosis with rare intraepidermal intercellular edema (spongiosis). The dermal infiltrate is composed of lymphocytes, monocytes, and mast cells with few or no eosinophils.
SPECIAL FORMS OF AD
Hand Dermatitis Aggravated by wetting and washing with detergents, harsh soaps, and disinfectants leads to ICD in the atopic. Clinically indistinguishable from “normal” ICD (see p. 21).
Exfoliative Dermatitis (see Section 8) Eryth roderma in patients with extensive skin involvement. Generalized redness, scaling, weeping, crusting, lymphadenopathy, fever, and systemic toxicity.
COMPLICATIONS
Secondary infection with S. aureus and HSV (eczema herpeticum, see Section 27). Rarely keratoconjunctivitis and corneal ulcers caused by HSV.
COURSE AND PROGNOSIS
Untreated involved sites persist for months or years. Spontaneous, more or less complete remission during childhood occurs in >40% with occasional recurrences during adolescence. In many patients, the disease persists for 15 to 20 years, but is less severe. Thirty to 50% of patients develop asthma and/or hay fever. Adult-onset AD exists and often runs a severe course. S. aureus infection leads to extensive erosions and crusting, and herpes simplex infection to eczema herpeticum, which may be life threatening (see Section 27).
MANAGEMENT
Education of the patient to avoid rubbing and scratching is most important. Use emollients. An allergic workup is rarely helpful in uncovering an allergen. However, in patients who are hypersensitive to house dust mites, various pollens, and animal hair proteins, exposure to the appropriate allergen may cause flares. AD may exacerbate with emotional stress and sweating. Patients should be warned of their special problems with herpes simplex and the superimposed staphylococcal infection. Acute
- Wet dressings and topical glucocorticoids; topical antibiotics (mupirocin ointment) when indicated.
- Hydroxyzine, 10 to 100 mg four times daily for pruritus.
- Oral antibiotics (cephalosporins, penicillins, doxycycline) to eliminate S. aureus and treat MRSA according to sensitivity as shown by culture.
Subacute and Chronic
- Hydration with unscented emollients (e.g., hydrated petrolatum) is a basic daily treatment to counteract xerosis; 12% ammonium lactate or 10% α-hydroxy acid lotion is very effective for xerosis. Soap showers are permissible for the body folds, but soap should seldom be used on the other parts of the skin surface.
- Topical anti-inflammatory agents such as glucocorticoids and calcineurin inhibitors are the mainstays of treatment. Of these,
glucocorticoids are the most effective. However, topical glucocorticoids may lead to skin atrophy if used for prolonged periods of time and if used excessively can potentially lead to suppression of the pituitary–adrenal axis. Another problem is “glucocorticoid phobia.” Patients or their parents are increasingly aware of glucocorticoid side effects and may refuse their use, no matter how beneficial they may be.
3. The calcineurin inhibitors, tacrolimus and pimecrolimus, are gradually replacing glucocorticoids in most patients. They potently suppress itching and inflammation and do not lead to skin atrophy. They are usually not effective enough to suppress acute flares, but work very well in minor flares and subacute AD.
4. Oral H1-antihistamines are useful in reducing itching.
5. Systemic glucocorticoids should be avoided, except in rare instances of severe intractable disease in adults: prednisone starting at 1 mg/kg, tapering over 2 to 3 weeks. Patients with AD tend to become dependent on oral glucocorticoids. Often, small
doses (5 to 10 mg) make the difference in control and can be reduced gradually to even 2.5 mg/d, as is often used for the control of asthma.
6. UVA–UVB phototherapy (combination of UVA plus UVB and increasing the radiation dose each treatment, with a frequency of two to three times weekly). Narrow band UV (311-nm) phototherapy and PUVA photochemotherapy are also effective.
7. In severe cases of adult AD and in normotensive healthy persons without renal disease, cyclosporine treatment (starting dose 5 mg/kg per day) is indicated when all other treatments fail, but should be monitored closely. Treatment is limited to 3 to 6 months because of potential side effects, including hypertension and reduced renal function. Blood pressure should be checked weekly and chemistry panels biweekly. Nifedipine can be used for moderate increases in blood pressure. Other treatment options include methotrexate, mycophenolate mofetil, azathioprine, and dupilumab.
8. Patients should learn and use stress management techniques.

FIGURE 2-12 • Atopic dermatitis: infantile Puffy face, confluent erythema, papules, microvesiculation, scaling, and crusting.

FIGURE 2-13 • Childhood atopic dermatitis A typical localization of atopic dermatitis in children is the region around the mouth. In this child, there is lichenification and fissuring as well as crusting.
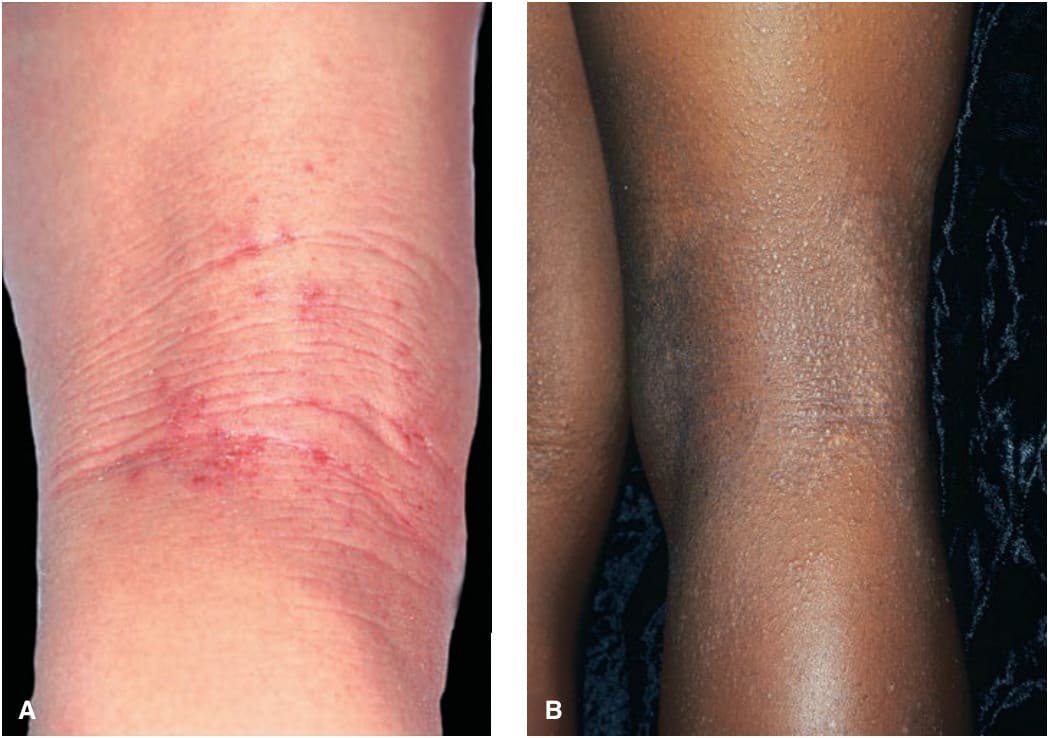
FIGURE 2-14 • (A) Childhood atopic dermatitis One of the hallmarks of atopic dermatitis is lichenification in the flexural regions as shown in this picture. Note the thickening of the skin with exaggerated skin lines and erosions. (B) Atopic dermatitis in African-American child. Pruritic follicular papules on posterior leg. Follicular eczema pattern is more common in African and Asian children.

FIGURE 2-15 • (A) Childhood atopic dermatitis This is a generalized eruption consisting of confluent, inflammatory papules that are erosive, excoriated, and crusted. (B) Adult atopic dermatitis Generalized eruption of follicular papules that are more heavily pigmented than normal skin in a 53-year-old woman of African extraction. There is extensive lichenification.
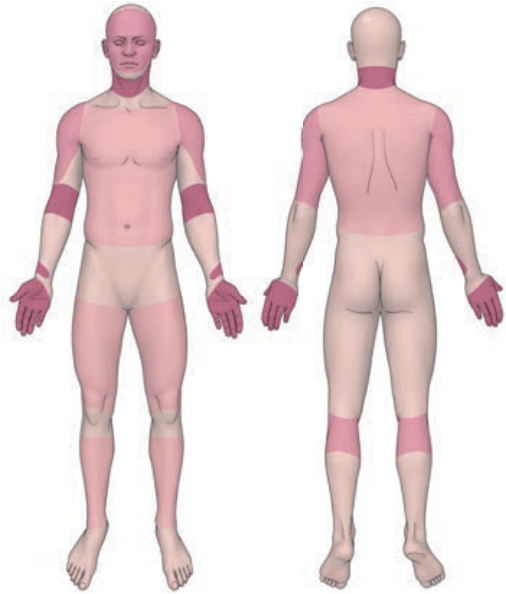
FIGURE 2-16 • Predilection sites of atopic dermatitis.

FIGURE 2-17 • Adult atopic dermatitis Lichenification may also affect the face and neck as in this 32-year-old woman. Skin is exceedingly thickened and there is temporal alopecia and loss of lateral eyebrows caused by rubbing. Note typical infraorbital fold (Dennie–Morgan sign).