ICHTHYOSIS VULGARIS
ICHTHYOSIS VULGARIS ICD-10: Q80.0
• Characterized by excessively dry skin with fine white to gray to brown scales.
• Affects extensors and torso.
• Frequently associated with atopy, hyperlinear palms and soles, keratosis pilaris.
EPIDEMIOLOGY
AGE OF ONSET Three to 12 months. SEX Equal incidence in males and females. Autosomal dominant inheritance. INCIDENCE Common (1 in 250).
PATHOGENESIS
Filaggrin mutation. Epidermis proliferates normally but keratin is retained with a resultant thickened stratum corneum.
CLINICAL MANIFESTATION
Very commonly associated with atopy. When hyperkeratosis is severe, many patients have a cosmetic concern.
SKIN LESIONS Xerosis (dry skin) with fine, powdery scaling but also larger, firmly adherent, tacked-down scales in a fish-scale pattern (Figs. 4-1 and 4-2). Diffuse general involvement, accentuated on the shins, arms, and back, buttocks, and lateral thighs; axillae and the antecubital and popliteal fossae spared (Figs. 4-2 and 4-3). The face is usually spared but the cheeks and forehead may be involved. Keratosis pilaris is perifollicular hyperkeratosis with little, spiny hyperkeratotic follicular papules of normal skin color either grouped or disseminated, mostly on the extensor surfaces of the extremities (Fig. 4-4); in childhood, also on cheeks. The hands and feet are usually spared, but palmoplantar markings are more accentuated (hyperlinear).
ASSOCIATED DISEASES More than 50% of individuals also have atopic dermatitis. There is also an increased risk of seasonal allergies, asthma and food allergies.
LABORATORY EXAMINATION
DERMATOPATHOLOGY Compact hyperkeratosis; reduced or absent granular layer; small, poorly formed keratohyalin granules by
Keratosis pilaris
electron microscopy, germinative layer flattened.
DIAGNOSIS
By clinical findings; absent or reduced keratohyalin granules in electron microscopy. Differential diagnosis includes all forms of xerosis and hyperkeratosis.
COURSE AND PROGNOSIS
Improvement in the summer, humid climates, and in adulthood. Keratosis pilaris occurring on the cheeks during childhood usually improves during adulthood.
MANAGEMENT
HYDRATION OF STRATUM CORNEUM Immersion in a bath followed by the application of petrolatum. Urea-containing creams bind water in the stratum corneum. KERATOLYTIC AGENTS Can help with scaling. α-Hydroxy acids (lactic acid or glycolic acid). Salicylic acid. Urea-containing creams and lotions (2% to 10%) are also effective. SYSTEMIC RETINOIDS Isotretinoin and acitretin are very effective, but careful monitoring for toxicity is required. Only severe cases may require intermittent therapy.

FIGURE 4-1 • Ichthyosis vulgaris: back Fine “fish scale”-like hyperkeratosis of the back.

FIGURE 4-2 • Ichthyosis vulgaris: legs Symmetric fine scale with “fish scale” appearance.
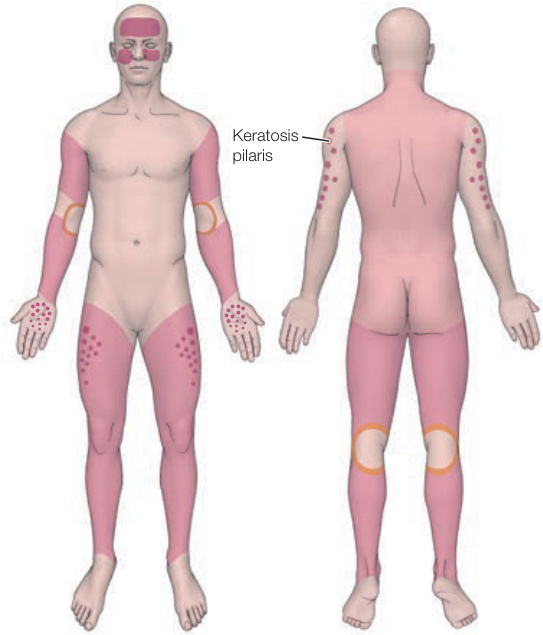
FIGURE 4-3 • Distribution of ichthyosis vulgaris Dots indicate keratosis pilaris. Palms with increased skin markings (hyperlinearity).
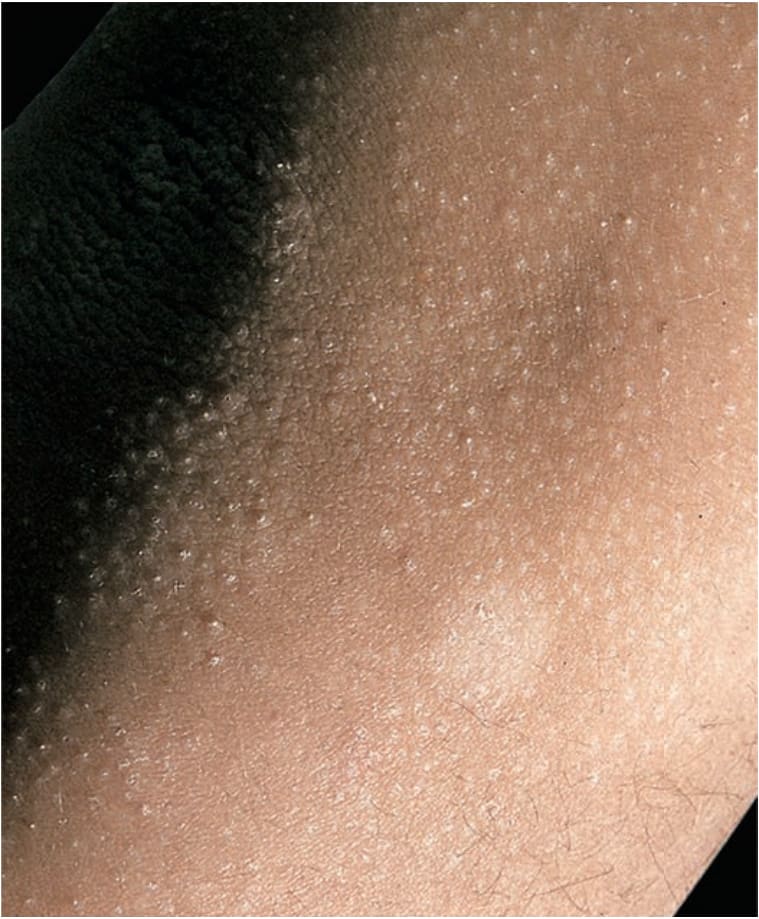
FIGURE 4-4 • Ichthyosis vulgaris. Keratosis pilaris: arm Small, follicular, horny spines occur as a manifestation of mild ichthyosis vulgaris; arising mostly on the shoulders, upper arms, and thighs. Desquamation of the nonfollicular skin results in hypomelanotic (less pigmented) spots similar to pityriasis alba (compare with Fig. 13-18).