DARIER DISEASE (DD)
DARIER DISEASE (DD) ICD-10: L87
• A rare autosomal-dominant inherited disease with onset during adolescence.
• Multiple discrete scaling, crusted, and pruritic papules mainly in seborrheic and flexural areas.
• Malodorous and disfiguring, also involving nails and mucous membranes.
• Itching and/or painful.
• Histologically characterized by suprabasal acantholysis and dyskeratosis.
• Caused by loss-of-function mutation in the ATP2A2 gene.
• Synonym: Darier–White disease, keratosis follicularis.
EPIDEMIOLOGY AND ETIOLOGY
Rare. AGE OF ONSET Usually in the first or second decade; males and females are equally affected. GENETICS Autosomal-dominant trait, penetrance >95%. Loss-of-function mutations in the ATP2A2 gene encoding, sarco/endoplasmic reticulum calcium adenosine triphosphatase isoform 2 (SERCA 2), which impair intracellular Ca2+ signaling. PRECIPITATING FACTORS Frequently worse in summer with heat and humidity; also
exacerbated by ultra violet B, mechanical trauma, and bacterial infections. May be associated with neuropsychiatric issues and type 1 diabetes.
CLINICAL MANIFESTATION
Abrupt episodes after precipitating factors; associated with severe pruritus and often pain. SKIN LESIONS Multiple discrete scaling of crusted, pruritic papules (Fig. 5-3); when scaling crust is removed, a slit-like opening becomes visible (Fig. 5-4). Confluence to large plaques covered by hypertrophic warty masses
that are malodorous, particularly in intertriginous areas. DISTRIBUTION Corresponding to the “seborrheic areas”: chest (Fig. 5-3), back, ears, nasolabial folds, forehead (Fig. 5-4), and the scalp; axilla, neck, and the groin. PALMS AND SOLES Multiple, flat, cobblestone-like papules. APPENDAGES Hair not involved, but permanent alopecia may result from extensive scalp involvement and scarring. Nails with white and red longitudinal bands, V-shaped nicks at edge. MUCOUS MEMBRANES White, centrally depressed papules on the mucosa of cheeks, hard and soft palate, and gums, “cobblestone” lesions.
DISEASE ASSOCIATION
Associated with acrokeratosis verruciformis (allelic with DD). Multiple, small flat-topped papules predominantly on the dorsa of the hands and feet.
LABORATORY EXAMINATION
DERMATOPATHOLOGY Dyskeratotic cells in the spinous layer (corps ronds) and stratum
corneum (grains); suprabasal acantholysis and clefts (lacunae); and papillary overgrowth of the epidermis and hyperkeratosis.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Diagnosis based on the history of familial involvement, clinical appearance, and histopathology. May be confused with seborrheic dermatitis, Grover disease, benign familial pemphigus (Hailey–Hailey disease), and pemphigus foliaceus. Acrokeratosis verruciformis: flat warts (verrucae planae juveniles).
COURSE AND PROGNOSIS
Persisting throughout life and not associated with cutaneous malignancies.
MANAGEMENT
Sunscreens, avoidance of friction and rubbing, antibiotic therapy (systemic and topical) to suppress bacterial infection, topical retinoids (tazarotene and adapalene), or, most effective, systemic retinoids (isotretinoin or acitretin). Low-dose naltrexone may also be helpful.

FIGURE 5-3 • Darier disease: chest Primary lesions are reddish-brown, scaling, and crusted papules that feel warty when stroked. Where crusts have been removed, there are slitlike erosions that are later covered by hemorrhagic crusts.
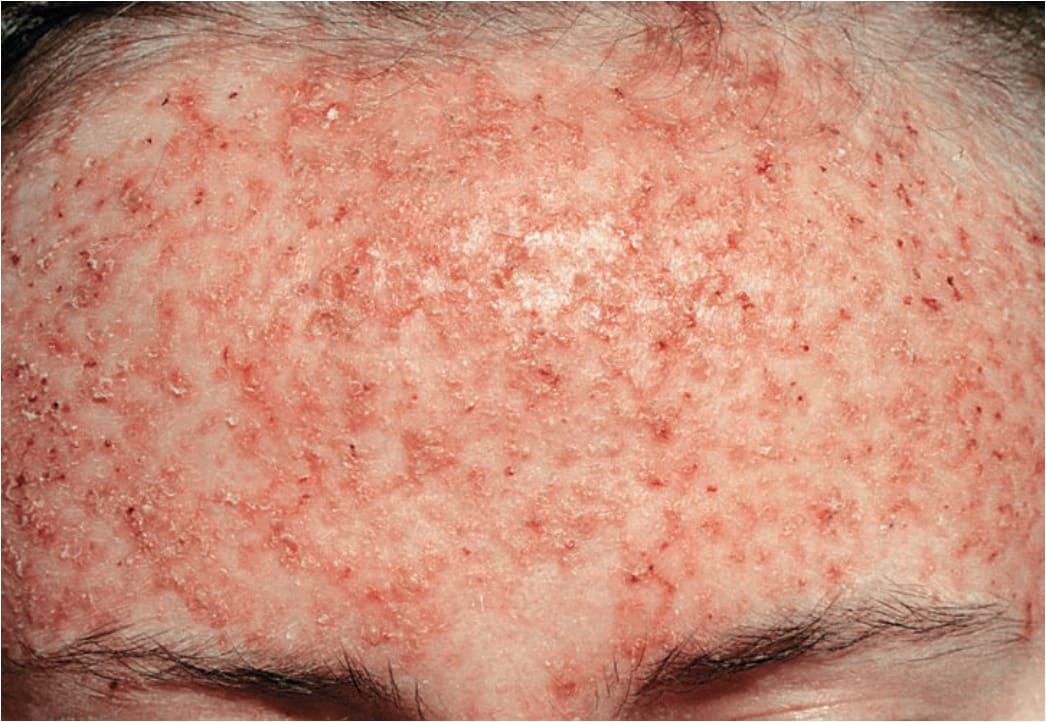
FIGURE 5-4 • Darier disease: forehead Partly coalescing, hyperkeratotic papules that are eroded and crusted. The main concern of this young female was disfigurement.