PEMPHIGUS
PEMPHIGUS ICD-10: L10
• A serious, acute or chronic, bullous autoimmune disease of skin and mucous membranes based on acantholysis.
• Two major types: Pemphigus vulgaris (PV) and pemphigus foliaceus (PF).
• PV: Flaccid blisters on skin and erosions on mucous membranes. PF: Scaly and crusted skin lesions.
• PV: Suprabasal acantholysis. PF: Subcorneal acantholysis.
• IgG autoantibodies to desmogleins, transmembrane desmosomal adhesion molecules.
• Serious and can be fatal, unless treated with immunosuppressive agents.
CLASSIFICATION (see Table 6-2) Epidemiology Pemphigus vulgaris (PV): Rare, more common in individual with Jewish and Mediterranean ancestry.
Pemphigus foliaceus (PF): Also rare but endemic in rural areas in of Brazil (fogo selvagem), where the prevalence can be as high as 3.4%. AGE OF ONSET Forty to 60 years; fogo selvagem also occurs in children and young adults.
IgG on cell surface of keratinocytesd IgG in cell surface patternd Desmoglein 3, sometimes desmoglein 1
Desmogleins 1, 3 (mucosal and skin involvement) Desmoglein 3 (mucosal dominant)
Desmoglein 1
Guinea pig esophagus or human skin substrate ideal IgG in intercellular pattern
Monkey esophagus substrate ideal IgG in cell surface pattern
Immunofluorescence
Suprabasal blister with acantholysis “row of tombstones” appearance IgG bound to surface of keratinocytes (intercellular pattern)
IgG bound to surface of keratinocytes (intercellular pattern)
Oral involvement is commond Suprabasal acantholysis, with papillomatosis of the dermal papillae and downward growth of epidermal strands into the dermis; presence of hyperkeratosis and scale-crust; eosinophilic or neutrophilic intraepidermal abscesses
Very rare Early lesions show eosinophilic spongiosis; histopathology demonstrates acantholysis below stratum corneum; epidermis beneath the granular layer remains intact; subcorneal pustules containing neutrophils and acantholytic epidermal cells in the blister cavity
Oral and nasal mucous membranes most commonly affected Esophageal Vulvar, cervical, vaginal Ocular
Pemphigus vulgaris Flaccid blisters, typically sparing palmoplantar surface Large erosions are common presentations (+) Nikolsky sign
Pemphigus foliaceus Scaly, crusted lesions on erythematous base; seborrheic distribution (face, scalp, upper trunk); small flaccid blisters are transient primary lesions
Pemphigus vegetansa Erosions develop excessive papillomatosis tissue and crusting; intertriginous areas, scalp, or face
Desmoglein 1e
Rare Similar to pemphigus foliaceus IgG and C3 deposition at granular basement membrane zone, IgG with intercellular pattern
Similar to pemphigus foliaceus; characterized by burning sensation, and exacerbation on sun exposure
Crusted lesions in seborrheic distribution
bVariant of pemphigus foliaceus.
aVariant of pemphigus vulgaris.
Endemic pemphigus foliaceus (fogo selvagem)c
Pemphigus erythema
tosusb
SEX Equal incidence in males and in females, but predominance of females with PF are in Tunisia and Colombia.
ETIOLOGY AND PATHOGENESIS
An autoimmune disorder. Loss of cell-to-cell adhesion in the epidermis (acantholysis). Occurs as a result of circulating antibodies of the IgG class, which bind to desmogleins, transmembrane glycoproteins in the desmosomes, members of the cadherin superfamily. Desmosomes hold epidermal cells (keratinocytes) together. In PV, desmoglein 3 (in some, also desmoglein 1). In PF, only desmoglein 1. Autoantibodies interfere with calcium- sensitive adhesion function and thus induce acantholysis.
CLINICAL MANIFESTATIONS
Pemphigus Vulgaris usually starts in the oral mucosa, but months may elapse before skin lesions occur. Less frequently, there may be a generalized, acute eruption of bullae from the beginning. No pruritus but burning and pain in erosions. Painful and tender mouth lesions may prevent adequate food intake. Epistaxis, hoarseness, and dysphagia. Weakness, malaise, and weight loss.
SKIN LESIONS Vesicles and bullae with serous content, flaccid (flabby) (Fig. 6-8), easily ruptured, and weeping (Fig. 6-9), arising on normal skin, randomly scattered, and discrete. Localized (e.g., to mouth or circumscribed skin area) or generalized with a random pattern. Extensive erosions bleed easily (Fig. 6-10), crusts particularly on scalp. Since blisters rupture so easily, only painful erosions in many patients.
Nikolsky Sign Dislodging of normal-appearing epidermis by lateral finger pressure in the vicinity of lesions, which leads to an erosion. Pressure on bulla leads to lateral extension of the blister.
Sites of Predilection Scalp, face, chest, axillae, groin, and umbilicus. In bedridden patients, there is extensive involvement of the back (Fig. 6-10). MUCOUS MEMBRANES Bullae are rarely seen in erosions of the mouth (see Section 33) and nose, pharynx and larynx, or vagina.
OTHER TYPES (see Table 6-2)
Pemphigus Vegetans (PVeg) A PV variant. Usually confined to intertriginous regions, perioral area, neck, and scalp. Granulomatous
vegetating purulent plaques that extend centrifugally. In these patients, there is a granulomatous response to the autoimmune damage of PV (Fig. 6-11).
Drug-Induced PV Clinically identical to sporadic PV. Several different drugs implicated, most significantly, captopril and D-penicillamine.
Pemphigus Foliaceus PF has no mucosal lesions and starts with scaly, crusted lesions on an erythematous base, initially in seborrheic areas. SKIN LESIONS Most commonly on the face, scalp, upper chest, and abdomen. Scaly, crusted erosions on an erythematous base (Fig. 6-12). In early or localized disease, sharply demarcated in seborrheic areas; they may stay localized or progress to generalized disease and exfoliative erythroderma. Initial lesion also a flaccid bulla, but this is rarely seen because of superficial location (see dermatopathology).
Brazilian Pemphigus (Fogo Selvagem) A distinctive form of PF endemic to south central Brazil. Clinically, histologically, and immunopathologically identical to PF. Patients improve when moved to urban areas but relapse after returning to endemic regions. Probably related to an arthropod-borne infectious agent, with clustering similar to that
of the black fly—simulium nigrimanum. More than 1000 new cases per year are estimated to occur in the endemic regions.
Pemphigus Erythematosus (PE) Synonym: Senear–Usher syndrome. A localized variant of PF largely confined to seborrheic sites. Erythematous, crusted, and erosive lesions in the “butterfly” area of the face, forehead, and presternal and interscapular regions. May have antinuclear antibodies.
Drug-Induced PF As in PV, associated with D-penicillamine and less frequently by captopril and other drugs. In most, but not all, instances, the eruption resolves after termination of therapy with the offending drug.
Neonatal Pemphigus Very rare, transplacental transmission from diseased mother; spontaneous resolution.
PARANEOPLASTIC PEMPHIGUS
This is a disease sui generis and is discussed in Section 19.
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY PV: Light microscopy (select early small bulla or, if not present, margin of larger bulla or erosion). Separation of keratinocytes, suprabasally, leading to split just above the basal cell layer and vesicles containing separated, rounded-up (acantholytic)
keratinocytes. PF: Superficial form with acantholysis in the granular layer of the epidermis. IMMUNOPATHOLOGY Direct immunofluorescence (IF) staining reveals IgG and often C3 deposited in lesional and perilesional skin in the intercellular substance of the epidermis. In PE Ig and complement deposits also found at the dermal epidermal junction. SERUM Autoantibodies (IgG) detected by indirect IF (IIF) or enzyme-linked immunoassay (ELISA). Titer usually correlates with activity of disease. In PV, autoantibodies against a 130-kDa glycoprotein, desmoglein 3, located in desmosomes of keratinocytes. In PF, autoantibodies to a 160-kDa intercellular (cell surface) antigen, desmoglein 1, in desmosomes of keratinocytes.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Differential diagnosis includes all forms of acquired bullous diseases (see Table 6-3). Differential diagnosis if only mouth lesions are present: aphthae, mucosal lichen planus, and erythema multiforme. Biopsy of the skin and mucous membrane, direct IF, and demonstration of circulating autoantibodies confirm a high index of suspicion.
COURSE
In most cases, the disease inexorably progresses to death unless treated aggressively with immunosuppressive agents. The mortality rate has been markedly reduced since treatment has become available. Currently, morbidity is mainly related to glucocorticoids and immunosuppressive therapies.
MANAGEMENT
Requires expertise and experience. Treatment to be performed by a dermatologist. GLUCOCORTICOIDS One to 2 mg/kg body weight of prednisone until cessation of new blister formation. Then rapid reduction to about half the initial dose until the patient is almost clear, followed by very slow tapering of the dose to the minimal effective maintenance dose. CONCOMITANT IMMUNOSUPPRESSIVE THERAPY Immunosuppressive agents are given concomitantly for their glucocorticoid-sparing effect:
Azathioprine. Most commonly prescribed nonsteroidal therapy prescribed for pemphigus. Check thiopurine methyl transferase levels before starting. 2.5 mg/kg
Disease Skin Lesions Mucous Membranes Distribution
PV Flaccid bullae on normal skin, erosions Almost always involved, erosions Anywhere, localized or generalized
PVeg Granulating plaques, occasionally vesicles at margin As in PV Intertriginous regions, scalp
PF Crusted erosions, occasionally flaccid vesicles Rarely involved Exposed, seborrheic regions or generalized
Bullous pemphigoid Tense bullae on normal and erythematous skin; urticarial plaques and papules
EBA Tense bullae and erosions, noninflammatory or BP-, DH- or LAD-like presentation
Mouth involved in 10%–35% Anywhere, localized or generalized
May be severely involved (oral esophagus, vagina)
Traumatized regions or random
Dermatitis herpetiformis Grouped papules, vesicles, urticarial plaques, crusted None Predilection sites: elbows, knees, gluteal, sacral, and scapular areas
Linear IgA dermatosis Annular, grouped papules, vesicles, and bullae Oral erosions and ulcers, conjunctival erosions and scarring
Anywhere
Disease Histopathology Immunopathology/ Skin Serum
PV Suprabasal acantholysis IgG intercellular pattern IgG AB to intercellular substance of epidermis (IIF) ELISA: AB to desmoglein 3 >>> desmoglein 1
PF Acantholysis in granular layer IgG, intracellular pattern IgG AB to intercellular substance of epidermis (IIF) ELISA: AB to desmoglein 1 only
PVeg Acantholysis ± intraepidermal neutrophilic abscesses, epidermal hyperplasia
As in PV As in PV
Bullous pemphigoid Subepidermal blister IgG and C3 linear at BMZ IgG AB to BMZ (IIF); directed to BPAG1 and BPAG2
EBA Subepidermal blister Linear IgG at BMZ IgG AB to BMZ (IIF) directed to type VII collagen (ELISA, Western blot)
Dermatitis herpetiformis Papillary microabscesses, subepidermal vesicle Granular IgA in tips of papillae Antiendomysial antibodies
Linear IgA dermatosis Subepidermal blister with neutrophils Linear IgA at BMZ Low titers of IgA AB against BMZ
AB, antibody; BMZ, basement membrane zone; BP, bullous pemphigoid; DH, dermatitis herpetiformis; EB, epidermolysis bullosa acquisita; ELISA, enzyme-linked immunosorbent assay; IIF, indirect immunofluorescence; LAD, linear IgA dermatosis; PF, pemphigus foliaceus; PV, pemphigus vulgaris; PVeg, pemphigus vegetans.
body weight for several months, then 50 mg maintenance dose. Myelosuppression, malignancy, and infections are potential side effects. Mycophenolate mofetil. Can by useful at doses of 2 to 3 g daily. Less severe side effect profile than azathioprine. Rituximab. Monoclonal antibody to CD20 targets B cells, the precursors of (auto) antibody-producing plasma cells. Consider adding to first line treatment in patients with moderate to severe involvement. Serious infections may be seen. Dapsone. Limited data suggest that doses of 50 to 200 mg daily may be helpful with
pemphigus foliaceus. Patients with glucose-6- phosphate dehydrogenase (G6PD) have an increased risk of severe hemolytic anemia. OTHER MEASURES Cleansing baths, wet dressings, topical and intralesional glucocorticoids, and antimicrobial therapy in documented bacterial infections. Correction of fluid and electrolyte imbalance. MONITORING Clinical, for improvement of skin lesions and development of drug-related side effects. Laboratory monitoring of pemphigus antibody titers and for hematologic and metabolic indicators of glucocorticoid- and/or immunosuppressive-induced adverse effects.

FIGURE 6-8 • Pemphigus vulgaris This is the classic initial lesion: flaccid, easily ruptured bulla on normal-appearing skin. Ruptured vesicles lead to erosions that subsequently crust as seen in the two smaller lesions.

FIGURE 6-9 • Pemphigus vulgaris Widespread confluent flaccid blisters on the lower back of a 40-year-old male who had a generalized eruption including scalp and mucous membranes. The eroded lesions are extremely painful.

FIGURE 6-10 • Pemphigus vulgaris Widespread confluent erosions that are very painful and bleed easily in a 53-year-old male. There are hardly any intact blisters because they are so fragile and break easily. The blood tracts go sideways because the patient had been lying on his right side before the photograph was taken.

FIGURE 6-11 • Pemphigus vegetans Papillomatous, cauliflower-like, oozing growths in the groin and pubis of a 50-year-old man.

FIGURE 6-12 • Pemphigus foliaceus Superficial erosions and crusted erythematous patches on the face, neck, and upper chest.
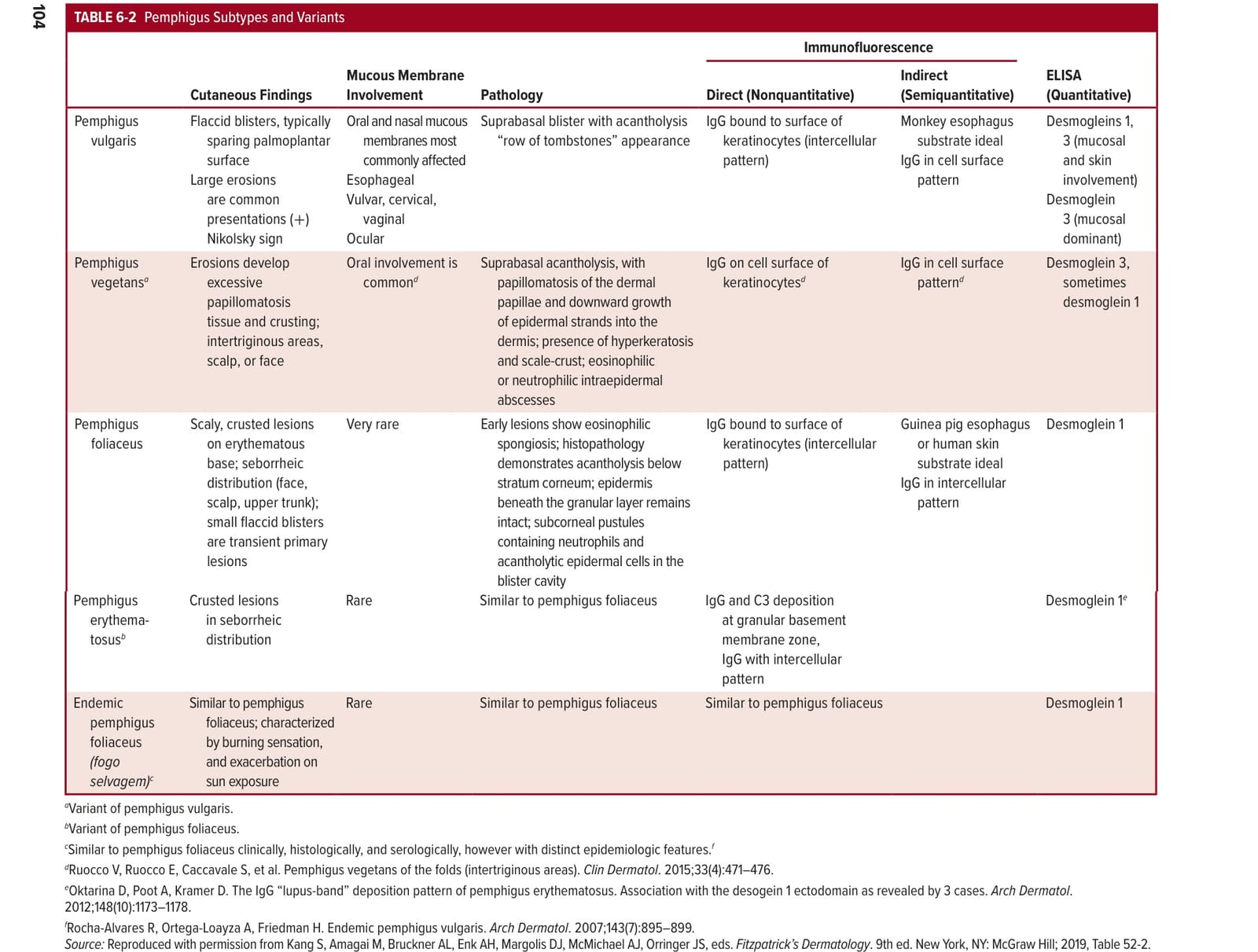
表 6-2
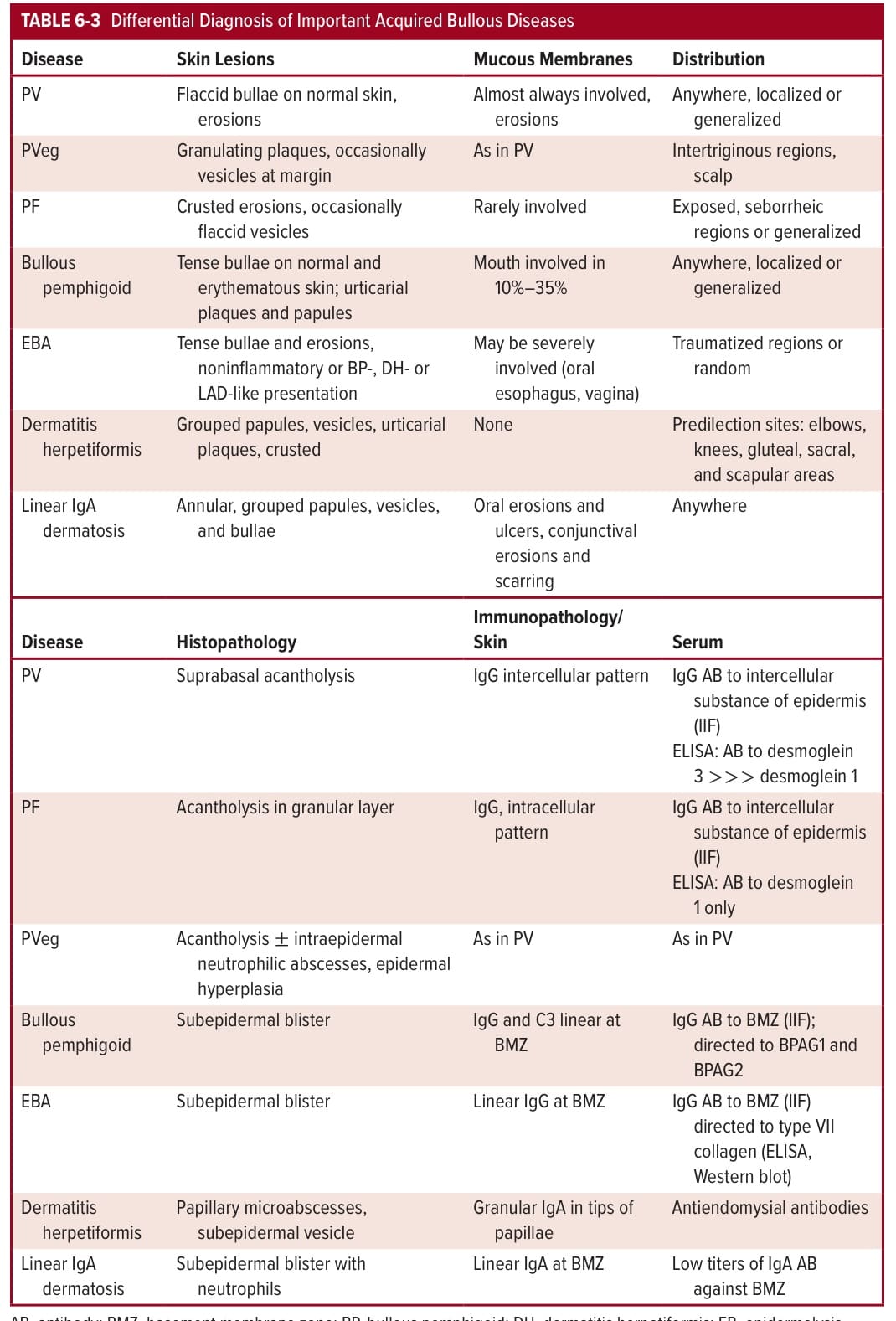
TABLE 6-3 Differential Diagnosis of Important Acquired Bullous Diseases