SWEET SYNDROME (SS)
SWEET SYNDROME (SS) ICD-10: L98.2
• An uncommon, acute, and recurrent, cytokine-induced skin reaction associated with various etiologies.
• Painful plaque-forming inflammatory papules, often with massive exudations giving the appearance of vesiculation (pseudovesiculation).
• Accompanied by fever, arthralgia, and peripheral leukocytosis.
• Associated with infection, malignancy, or drugs.
• Treatment: Systemic glucocorticoids, potassium iodide, dapsone, or colchicine.
• Synonym: Acute febrile neutrophilic dermatosis.
EPIDEMIOLOGY AND ETIOLOGY
AGE OF ONSET Most often 30 to 60 years. SEX Women > men. ETIOLOGY Unknown, possibly hypersensitivity reaction. It belongs to the group of neutrophilic dermatoses and possibly to the spectrum of autoinflammatory diseases. ASSOCIATED DISORDERS Upper respiratory tract and gastrointestinal infections (usually occurs 1 to 3 weeks after infection), pregnancy, and inflammatory bowel disease. May precede, follow, or appear concurrently as malignancy (hematologic > solid tumors). Can also occur with drugs: granulocyte colony-stimulating factor (G-GSF), ipilimumab.
CLINICAL MANIFESTATION
Prodromes are febrile upper respiratory tract infections. Gastrointestinal symptoms (diarrhea), tonsillitis, influenza-like illness, 1 to 3 weeks before skin lesions. Lesions tender/ painful. Fever (not always present), headache, arthralgia, and general malaise. SKIN LESIONS Bright red, smooth, tender papules (2 to 4 mm in diameter) that coalesce to form irregular, sharply bordered, inflammatory plaques (Fig. 7-6A). Pseudovesiculation: Intense edema gives the appearance of vesiculation (Figs. 7-6A and 7-7A). Lesions arise rapidly, and as they evolve, central clearing
may lead to annular or arcuate patterns. Tiny, superficial pustules may occur. May present as a single lesion or multiple lesions, asymmetrically or symmetrically distributed. Most common on face (Fig. 7-6A), neck (Fig. 7-6B), and upper extremities but also on lower extremities, where lesions may be deep in the fat and thus mimic panniculitis. Truncal lesions are uncommon but widespread and generalized forms occur. If associated with leukemia, bullous lesions may occur (Fig. 7-7B) and lesions may mimic bullous PG. MUCOUS MEMBRANES ± Conjunctivitis, episcleritis.
General Examination Patient may appear ill. There may be involvement of cardiovascular, central nervous system, gastrointestinal, hepatic, musculoskeletal, ocular, pulmonary, renal, and splenic organs.
LABORATORY EXAMINATIONS
COMPLETE BLOOD COUNT Leukocytosis with neutrophilia (not always present). ESR Elevated. DERMATOPATHOLOGY Diagnostic. Epidermis usually normal, sometimes subcorneal pustulation. Massive edema of papillary body, dense leukocytic infiltrate with starburst pattern in mid-dermis, consisting of neutrophils with occasional eosinophils/lymphoid cells. Leukocytoclasia,
A
B
A B
nuclear dust, but no vasculitis. ± Neutrophilic infiltrates in subcutaneous tissue.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Clinical impression and by histopathology. DIFFERENTIAL DIAGNOSIS Erythema multiforme, erythema nodosum, prevesicular herpes simplex infection, preulcerative PG.
COURSE AND PROGNOSIS
Untreated, lesions enlarge over a period of days or weeks and eventually resolve without
scarring. Recurrences occur in 30% to 69% of patients, often in previously involved sites and more often when associated with malignancy.
MANAGEMENT
Rule out sepsis. PREDNISONE First-line treatment (0.5 to 1 mg/kg), ideally tapering over 4 to 6 weeks. Lesions typically improve within a few days. ALTERNATIVE THERAPY Colchicine, dapsone, potassium iodide.

FIGURE 7-6 • Sweet syndrome (A) An erythematous, edematous plaque that has formed from coalescing papules on the right cheek. The border of the plaque looks as if composed of vesicles, but palpation reveals that it is solid (pseudovesiculation). This lesion occurred in a 26-year-old female following an upper respiratory infection, and the patient also had fever and leukocytosis. (B) A more exanthematic eruption in a 23-year-old female. There are multiple, coalescing, inflammatory, and very exudative papules with a wheal-like appearance on the neck. This patient also had leukocytosis and fever.
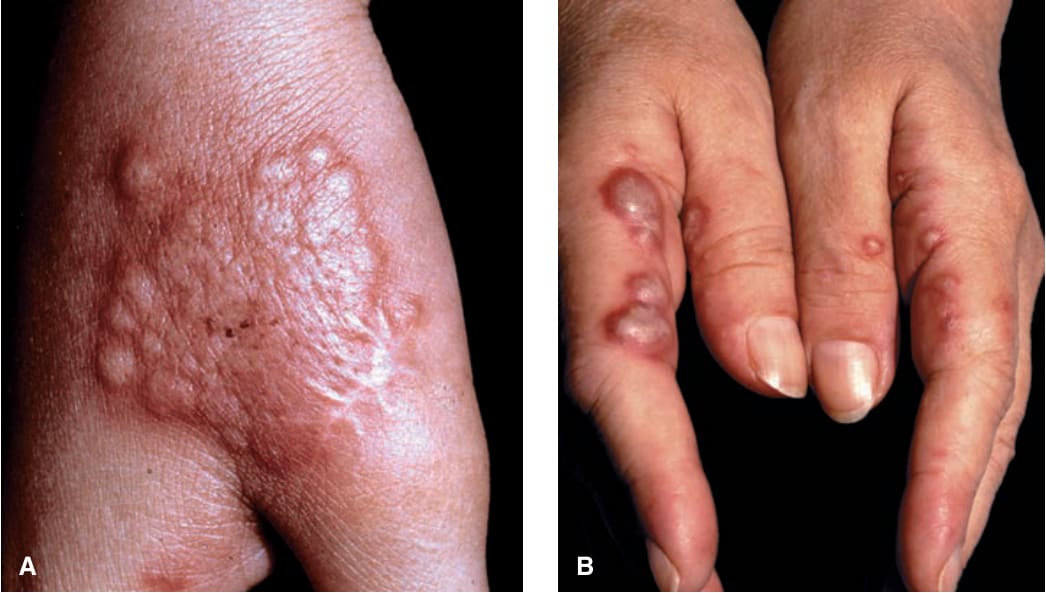
FIGURE 7-7 • Sweet syndrome (A) Coalescing exudative papules that look like vesicles. Upon palpation, lesions were solid. (B) Bullous type of Sweet syndrome. These are true bullae and pustules. The patient had myelomonocytic leukemia.