ERYTHEMA NODOSUM (EN) SYNDROME
ERYTHEMA NODOSUM (EN) SYNDROME ICD-10: L52
• EN is an important and common acute inflammatory/immunologic reaction pattern of the subcutaneous fat.
• Characterized by the appearance of painful nodules on bilateral shins.
• Lesions are bright red and flat but nodular upon palpation.
• Often fever and arthritis.
• Multiple and diverse etiologies.
The most common type of panniculitis, with a peak incidence at 20 to 30 years, but any age may be affected. Three to six times more common in females than in males. ETIOLOGY Erythema nodosum (EN) is cutaneous reaction pattern to various etiologic agents. These include infections, drugs, and other inflammatory/granulomatous diseases, notably sarcoidosis (Table 7-1).
CLINICAL MANIFESTATION
Painful, tender lesions, usually of a few days’ duration, accompanied by fever, malaise, and arthralgia (50%), most frequently of
ankle joints. Other symptoms depending on etiology. SKIN LESIONS Indurated, very tender nodules (2 to 5 cm), not sharply marginated (Fig. 7-9), deep seated in the subcutaneous fat, mostly on the anterior lower legs, bilateral but not symmetric. Nodules are bright to deep red and are appreciated as such only upon palpation. The term erythema nodosum best describes the skin lesions: they look like erythema but feel like nodules (Fig. 7-9). Lesions are oval, round, and arciform; as they age, they become violaceous, brownish, yellowish, or green, like resolving hematomas. Lesions may also occur
Bacterial Infections
● Streptococcal infections
● Tuberculosis
● Yersinia infections
● Salmonella infections
● Campylobacter infections
● Brucellosis
● Tularemia
● Atypical mycobacterial infections
● Chancroid
● Meningococcemia
● Corynebacterium diphtheriae infections
● Cat-scratch disease
● Propionibacterium acnes
● Shigella infections
● Gonorrhea
● Syphilis
● Leptospirosis
● Q fever
● Lymphogranuloma venereum
● Chlamydophila psittaci infections
● Mycoplasma pneumoniae infections
● Helicobacter pylori infection
Viral Infections
● Infectious mononucleosis
● Hepatitis B
● Milker nodules
● Orf (contagious ecthyma)
● Herpes simplex
● Measles
● Cytomegalovirus infections
Fungal Infections
● Dermatophytes
● Blastomycosis
● Histoplasmosis
● Coccidioidomycosis
● Sporotrichosis
● Aspergillosis
Protozoal Infections
● Toxoplasmosis
● Ancylostomiasis
● Amebiasis
● Giardiasis
● Ascariasis
Drugs
● Sulfonamides
● Bromides
● Iodides
● Oral contraceptives, progesterone
● Minocycline
● Gold salts
● Penicillin
● Salicylates
● Chlorothiazides
● Phenytoin
● Aminopyrine
● Arsphenamine
● Hepatitis B vaccine
● Nitrofurantoin
● Pyritinol
● D-Penicillamine
● Thalidomide
● Isotretinoin
● Interleukin-2
● Omeprazole
● Valproate
● Tdap (tetanus, diphtheria, and pertussis) vaccine
● Leukotriene-modifying agents
● Vemurafenib Miscellaneous Conditions
● Sarcoidosis
● Ulcerative colitis
● Colon diverticulosis
● Crohn disease
● Behçet disease
● Reactive arthritis
● Sweet syndrome
● Pregnancy
● Takayasu arteritis
● Immunoglobulin A nephropathy
● Chronic active hepatitis
● Granulomatous mastitis
● Vogt–Koyanagi disease
● Sjögren syndrome
● Temporal arteritis
● Systemic lupus erythematosus
● Dental infection
Malignant Diseases
● Hodgkin disease
● Non-Hodgkin lymphoma, including mucosaassociated lymphoid tissue (MALT) lymphoma
● Leukemia
● Sarcoma
● Renal carcinoma
● Postradiotherapy for pelvic carcinoma
Source: Reproduced with permission from Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, Orringer JS, eds. Fitzpatrick’s Dermatology. 9th ed. New York, NY: McGraw Hill; 2019, Table 73-3.
on the knees and arms but only rarely on the face and neck.
LABORATORY EXAMINATIONS
HEMATOLOGY Elevated ESR and C-reactive protein; leukocytosis. BACTERIAL CULTURE Culture throat for group A β-hemolytic streptococcus.
IMAGING Radiologic examination of the chest is important to rule out sarcoidosis or other pulmonary disease. DERMATOPATHOLOGY Acute (polymorphonuclear) and chronic (granulomatous) inflammation in the subcutis, around blood vessels in the septum and adjacent fat. EN is a septal panniculitis.
COURSE
Most cases spontaneously resolve in 6 weeks, though up to one-third may recur. Lesions do not ulcerate, and heal without scarring.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Diagnosis rests on clinical criteria and histopathology, if needed. Differential diagnosis includes all other forms of panniculitis,
nodular vasculitis, pretibial myxedema, urticaria, and lymphoma.
MANAGEMENT
SYMPTOMATIC Bed rest, leg elevation, compressive bandages (lower legs). ANTI-INFLAMMATORY TREATMENT Nonsteroidal anti-inflammatory drugs are the first line treatment. Colchicine, dapsone, and potassium iodide can also be used. Systemic glucocorticoids can provide rapid improvement in patients with severe disease.
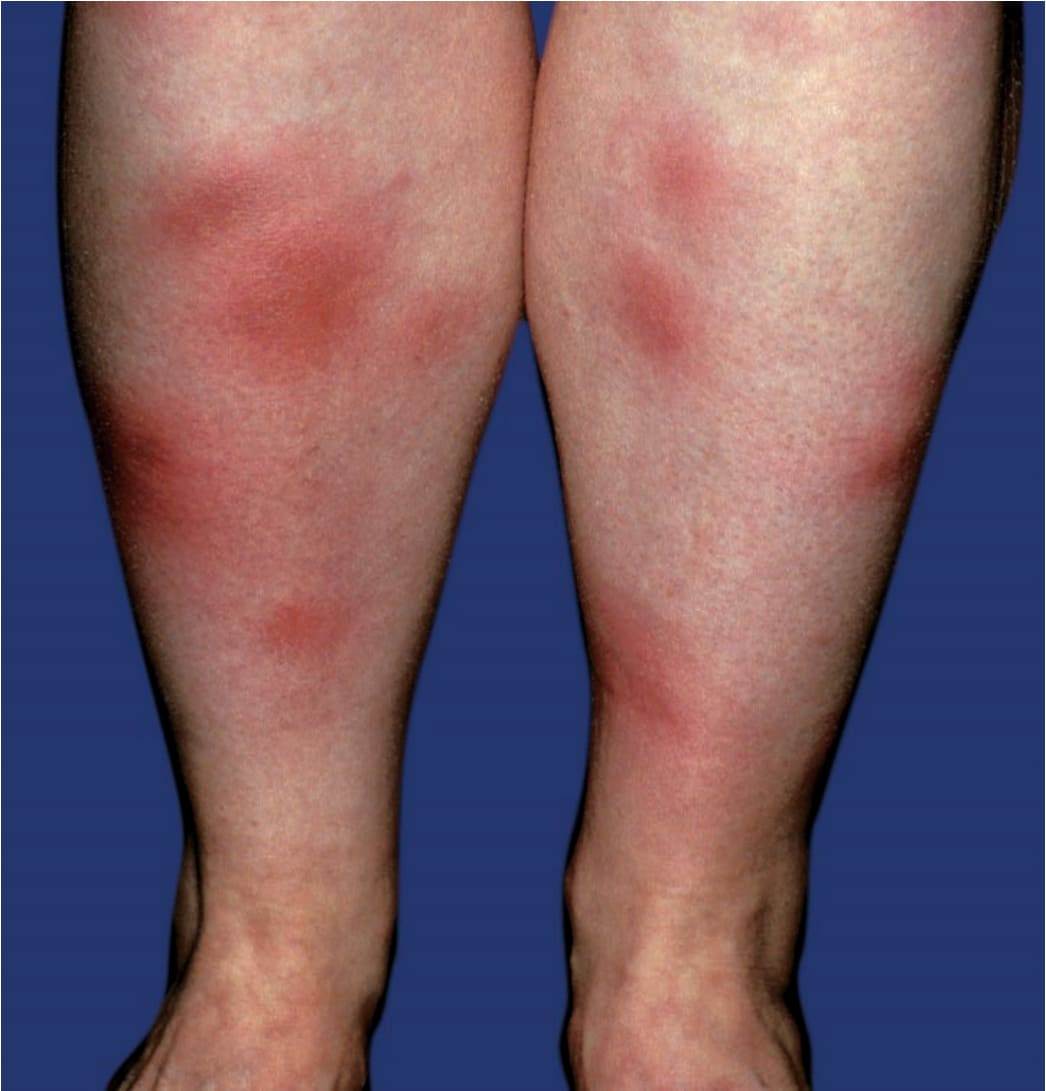
FIGURE 7-9 • Erythema nodosum Indurated, very tender, inflammatory nodules mostly in the pretibial region. Lesions are seen as red, ill-defined erythemas but palpated as deep-seated nodules, hence the designation. In this 49-year-old female, there was also fever and arthritis of the ankle joints following an upper respiratory tract infection. The throat cultures yielded β-hemolytic streptococci.
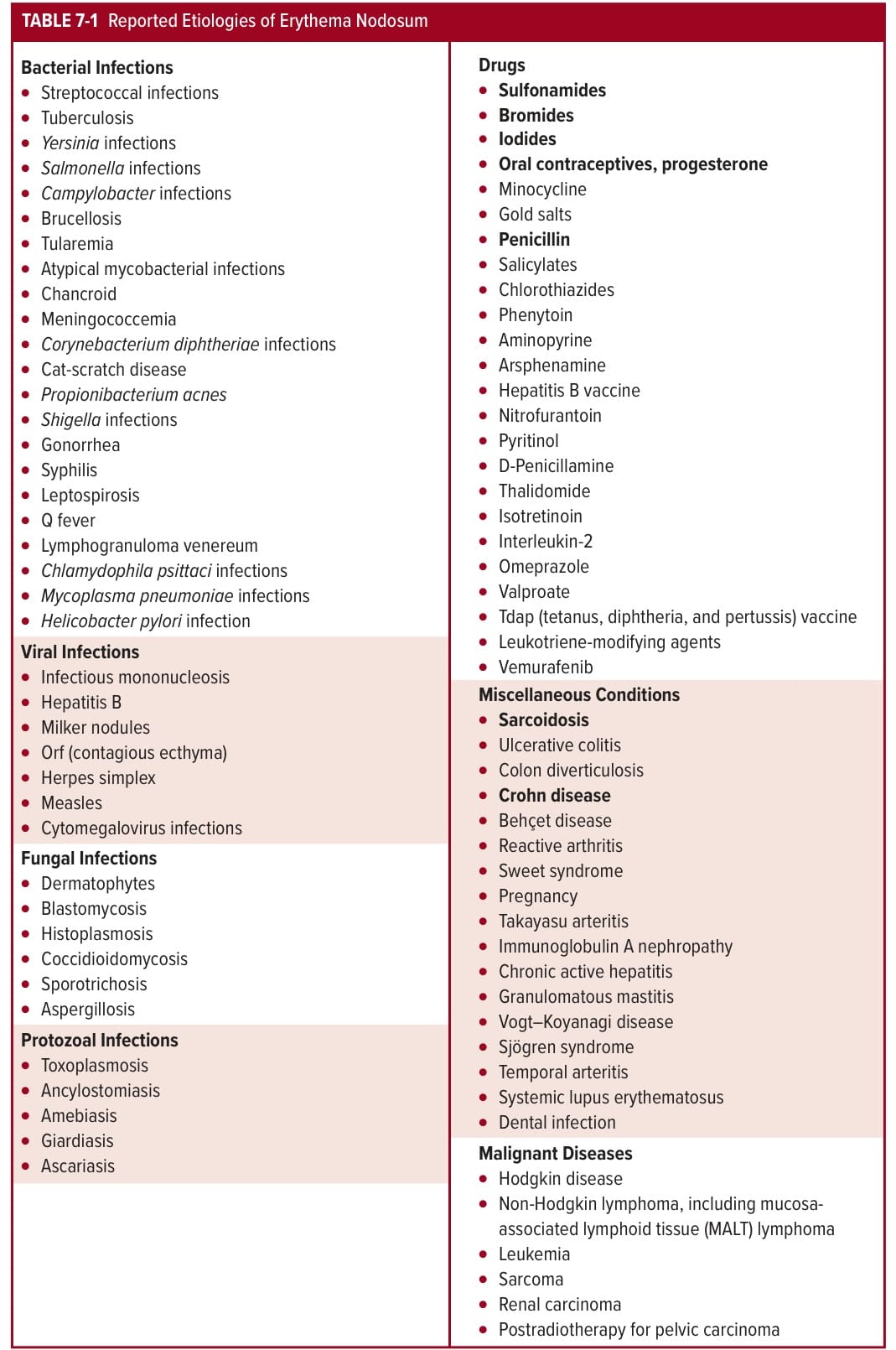
TABLE 7-1 Reported Etiologies of Erythema Nodosum