OTHER PANNICULITIDES
OTHER PANNICULITIDES ICD-10: M79.3
• Panniculitis is the term used to describe diseases where the major focus of inflammation is in the subcutaneous tissue. In general, panniculitis presents as an erythematous or violaceous nodule in the subcutaneous fat that may be tender or not, may ulcerate or heal without scarring, and may be soft or hard on palpation. Thus, the term panniculitis describes a wide spectrum of disease manifestations.
• An accurate diagnosis requires an ample deep skin biopsy that should reach down to, or even beyond, the fascia. The panniculitides are classified histologically as lobular or septal but a clear separation is often not possible. A simplified classification of panniculitis is given in Table 7-2.
• Only two forms of panniculitis are briefly discussed here.1 Other diseases in which panniculitis occurs are referred to in Table 7-2.
• Pancreatic panniculitis manifests as painful erythematous nodules and plaques that may fluctuate and occur at any site, with a predilection for abdomen, buttocks, and legs (Fig. 7-10). Frequently accompanied by arthritis and polyserositis. Associated with pancreatitis or pancreatic carcinoma. In middle-aged to elderly individuals, males > females. History: alcoholism, abdominal pain, weight loss, or recent-onset diabetes mellitus. Skin biopsy reveals lobular panniculitis; liquefied fat may drain from the biopsy site. General examination may reveal pleural effusion, ascites, and arthritis, particularly of the ankles. Laboratory: Eosinophilia, hyperlipasemia, hyperamylasemia, and increased excretion of amylase and/or lipase in the urine. The pathophysiology is probably a breakdown of subcutaneous fat caused by pancreatic enzymes released into the circulation. Course and prognosis depend on the type of pancreatic disease. Treatment is directed at the underlying pancreatic disorder.
• α1-Antitrypsin-deficiency panniculitis is also characterized by recurrent tender, erythematous, subcutaneous nodules ranging from 1 to 5 cm and located predominantly on the trunk and the proximal extremities. Nodules break down and discharge a clear serous or oily fluid. Diagnosis is substantiated by a decrease of serum α1-antitrypsin, and treatment consists of oral dapsone in doses up to 200 mg/d. The intravenous infusion of human α1-proteinase inhibitor concentrate has been shown to be very effective.
1The reader is also referred to Aronson IK et al., in Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, Orringer JS (eds.): Fitzpatrick’s Dermatology in General Medicine 9th edition. New York, NY: McGraw-Hill: 2019.
Compression therapy is the major recommended treatment (30–40 mm Hg) Stanozolol: to decrease pain, erythema, induration Pentoxifylline, horse chestnut seed extract, oxerutins, flavonoid fraction Weight loss
Bed rest, aspirin, NSAIDs SSKI, 2–10 drops thrice daily Colchicine Corticosteroids (rarely indicated)
If MTB testing is positive, full course of multidrug therapy Treat underlying cause SSKI, NSAIDs, colchicine, antimalarials, corticosteroids, gold Bed rest Pentoxifylline, compression
Lobular, often with vasculitis (90%). Early central necrosis of adipocytes; neutrophilic infiltrate In older lesions, epithelioid histiocytes, multinucleated giant cells
Stasis changes Lobular panniculitis No vasculitis Ischemic necrosis at center Thickened, fibrotic septa, atrophy of subcutaneous fat Membranocystic changes
Septal Panniculitis No vasculitis Neutrophils (early), Meischer granulomas (late)
Erythematous SQ nodules on lower extremities May affect calves, anterolateral leg Tenderness, ulceration, scarring Protracted course, with recurrent episodes 3–6 weeks duration
Acute onset; symmetric, tender, nodules and plaques Affecting anterior lower extremities Fever, fatigue, arthralgias, arthritis, headache, no ulceration, no atrophy, no scarring
Indurated, woody plaques on lower extremities, with acute and chronic changes (most commonly, anteromedial calf area) Intense pain is the most frequent symptom Stage: acute inflammatory Chronic fibrosis Inverted champagne bottle
Erythema nodosum Young women, 2nd to 4th decades Infections (commonly streptococcal), medications, malignancies (leukemias, lymphomas)
Erythema induratum Young/middle-aged women Venous insufficiency, obesity Infectious etiology: MTB, hepatitides B, C
Overweight women older than 40 years Venous insufficiency Obesity Systemic sclerosis Pulmonary Infarction Hypertension
Lipodermatosclerosis (sclerosing panniculitis, hypodermitis sclerodermiformis, chronic panniculitis with lipomembranous changes, sclerotic atrophic cellulitis, venous stasis panniculitis)
(Continued)
MILD–MODERATE: dapsone, doxycycline SEVERE: protein replacement therapy
Depends on the known organisms
Octreotide Plasmapheresis
Mostly lobular panniculitis, but with a mixed pattern Pattern dependent on whether infection was inoculation related or hematogenous Neutrophilic infiltrate
Lobular panniculitis No vasculitis Intense necrosis at center of lobule Ghost adipocytes Saponification and calcification
Early necrosis of SQ fat Splaying of neutrophils between collagen bundles is characteristic Liquefactive necrosis
Erythematous plaques, nodules, abscess with purulent discharge (fluctuant/abscess-type lesions) Most commonly on legs and feet Upper extremities, trunk, face may be involved
Pancreatitis, pancreatic CA Erythematous nodules with spontaneous ulceration Lower extremities, especially periarticular areas (knee, ankle) Crops of lesions; red–brown Atrophic, hyperpigmented scarring Oily abscesses
Painful erythematous nodules and plaques Cellulitis, fluctuant abscess type Most common site: lower trunk, also buttocks, proximal extremities May be life-threatening
Infectious panniculitis — Wide variety of bacteria, fungi, parasites, viruses Either primarily inoculated, or hematogenous Staphylococcus aureus panniculitis with juvenile diabetes Panniculitis of mycetoma, chromoblastomycosis, sporotrichosis
Pulmonary and hepatic disease (emphysema in COPD, cirrhosis, hepatocellular CA), highest risk ZZ phenotype Panniculitis uncommon in AAT deficiency
Pancreatic panniculitis Occurs in 2%–3% of patients with pancreatic disorders
α1-Antitrypsin panniculitis Most common in 30–60 years of age groups MM: most common phenotype (normal AAT) ZZ: 10%–15% of N levels; associated with >60% of cases
Hydroxychloroquine is firstline treatment Quinacrine
Corticosteroids Cyclosporine Multidisciplinary care in a hospital setting
Corticosteroids alone, or corticosteroids with methotrexate
Mixed septal and lobular panniculitis, lymphocytic and plasma cell infiltrate, hyaline sclerosis of septal collagen; calcification, membranocystic changes in late stages
Vacuolar alteration of basal cell layer, thickened basement membrane, mucin deposition, superficial and deep perivascular infiltrate Mostly lobular panniculitis, with lymphoid follicles, variable hyaline fat necrosis, sclerotic collagen bundles, lymphocytic and plasma cell infiltrate
Lobular panniculitis No vasculitis Bean bag cells: macrophages with intact or fragmented erythrocytes, leukocytes, or platelets Necrosis
UPPER ARMS (lateral), shoulders, face, scalp, hips, buttocks, breasts Rare on lower extremities Deep, tender SQ nodules; no surface changes Resolves with depressed lipoatrophic areas Chronic, with yearly/periodic flares Duration: average of 6 years
HLH MAS SQ erythematous to violaceous plaques on extremities, trunk Fulminant cases may have: ulceration, fever, hepatosplenomegaly, hemocytophagocytosis in BM, LN, liver, CNS May be acute and intermittent, or have a rapidly fatal course
Panniculitis with dermatomyositis Very rare Dermatomyositis Erythematous nodules and plaques, affecting arms, buttocks, thighs, abdomen
Systemic lupus erythematosus SjÖgren syndrome Rheumatoid arthritis
Lupus panniculitis Females more frequently affected than males (4:1) 30–60 years old, also in childhood May occur before or after diagnosis of lupus erythematosus or discoid lupus erythematosus
Cytophagic histiocytic panniculitis Rare; seen in adults, adolescents, and children
Spontaneous resolution Monitor serum calcium for hypercalcemia Systemic glucocorticoids may be considered; nephrocalcinosis
Psychiatric treatment; Intralesional steroids, surgical excision
Spontaneous resolution
Lobular panniculitis No vasculitis Suppurative granuloma involving fat lobule Refractile foreign material
Lobular panniculitis No vasculitis Needle-shaped clefts in radial array Nodules and plaques, resolving spontaneously
Lobular panniculitis No vasculitis Perivascular lymphohistiocytic infiltrate
Indurate, erythematous plaques or nodules at sites of cold exposure; affects face, thighs, scrotal fat of prepubertal boys Resolution within 3 months
Erythematous to violaceous, firm nodules or plaques affecting buttocks, back, shoulders, cheeks, thighs Anterior trunk spared Oily/chalky white material Late hypercalcemia (monitor for 6 months)
Factitial panniculitis — Associated with personality aberrations SQ implantation (medications, cosmetic fillers, oils, human waste)
Subcutaneous fat necrosis of the newborn Rare, first few weeks of life History of perinatal complications (meconium aspiration, hypothermia, hypoxemia, gestational diabetes)
Cold panniculitis (Haxthausen disease) Scrotal cold panniculitis in 9–14-year-old males Exposure to cold weather, popsicles, ice packs, swimming
A
B

FIGURE 7-10 • Pancreatic panniculitis (A) There is a painful, erythematous nodule that fluctuates on the ventral malleolar region but similar lesions were also found on the trunk and on the buttocks. (B) Painful erythematous yellow-brown fluctuant nodule in a 62-year-old man. See video of nodule drainage revealing a thin jelly-like exudate.
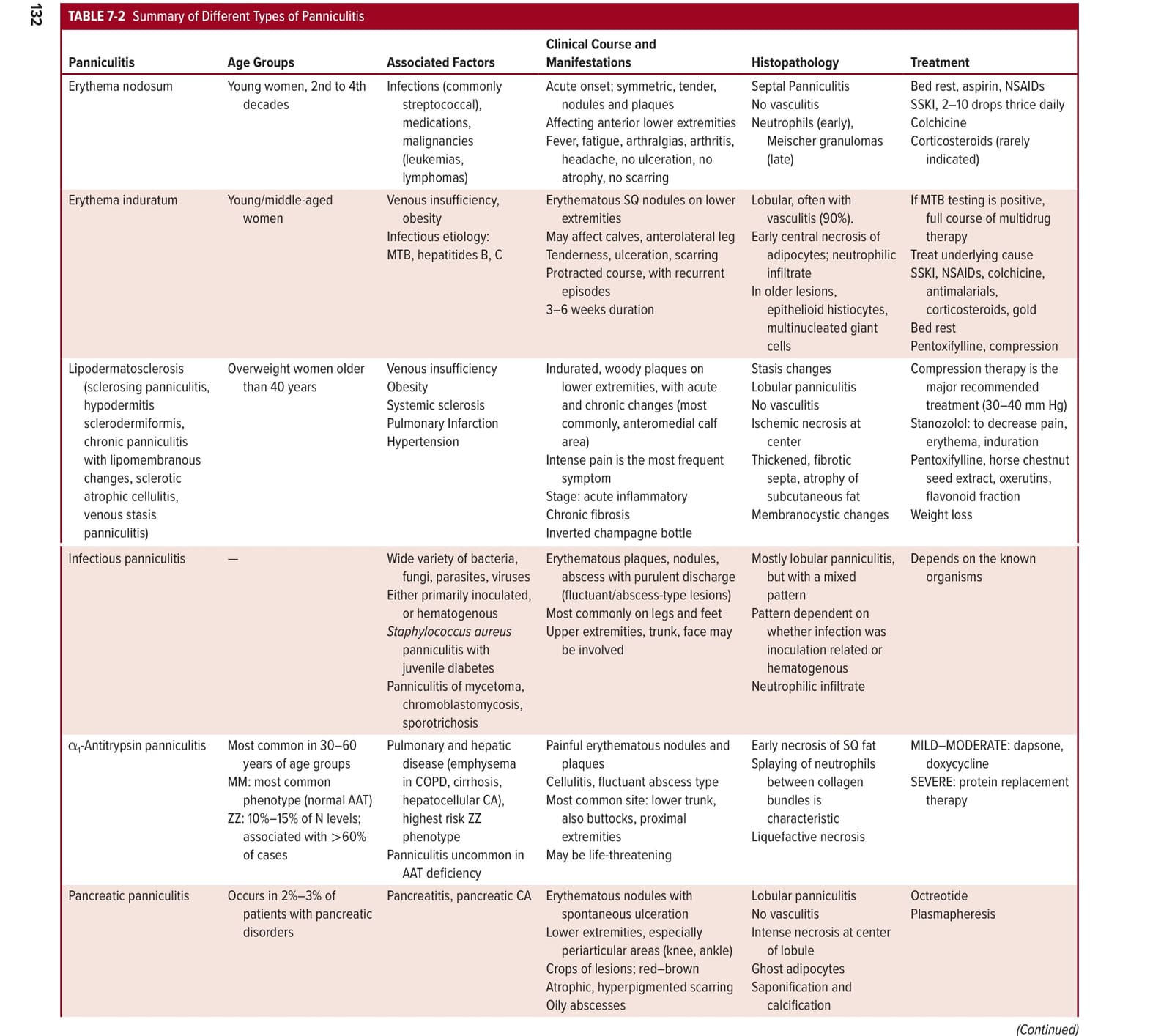
表 7-2