ACQUIRED MELANOCYTIC NEVI
ACQUIRED MELANOCYTIC NEVI ICD-10: D22.L10
• Melanocytic nevi commonly called moles, are very common, acquired pigmented macules, papules, or nodules.
• Composed of groups of melanocytic nevus cells located in the epidermis and dermis.
• They are benign tumors arising as nevus cell clusters at the dermal–epidermal junction (junctional melanocytic nevi), in combination with the papillary dermis (compound melanocytic nevi), or exclusively in the dermis (dermal melanocytic nevi).
EPIDEMIOLOGY AND ETIOLOGY
One of the most common acquired new growths in Caucasians (most adults have about 20 nevi), though patients with the lightest skin and red hair tend to have fewer nevi. Also less common in persons with more pigmented skin. RACE Blacks and Asians have more nevi on the palms, soles, and nail beds. HEREDITY Common acquired melanocytic nevi can occur in family clusters. SUN EXPOSURE A likely factor in the induction of nevi on the exposed areas, especially when intermittent and intense. SIGNIFICANCE Risk of melanoma is related to the number of acquired melanocytic nevi.
CLINICAL MANIFESTATION
DURATION AND EVOLUTION OF LESIONS Melanocytic nevi appear in early childhood and reach a maximum in young adulthood even though some lesions arise in adulthood. Later on, there is a gradual involution and fibrosis of lesions, but most disappear after the age of 60. In contrast, dysplastic nevi continue to
appear throughout life and are believed not to involute (see Section 12). SKIN SYMPTOMS Melanocytic nevi are asymptomatic. However, these nevi grow, and growth can be accompanied by itching. Itching per se is not a sign of malignancy, but if a lesion persistently itches or is tender, it should be followed carefully or biopsied, since persistent pruritus may be an early indication of malignant change.
CLASSIFICATION
Melanocytic are multiple (Fig. 9-1A) and can be classified according to the histologic level of the nevus cell clusters (Fig. 9-1B).
- Junctional melanocytic nevi: These arise at the dermal–epidermal junction, on the epidermal side of the basement membrane (Figs. 9-1B and 9-2).
- Compound melanocytic nevi: Nevus cells invade the papillary dermis, and nevus cell nests are now found both intraepidermally and dermally (Figs. 9-1B and 9-3).
- Dermal melanocytic nevi: These represent the last stage of the evolution of melanocytic nevi. “Dropping off” into the dermis
A
B Junctional MN Compound MN Dermal MN
A B
C D
is now completed, and the nevus grows or remains intradermal (Figs. 9-1B and 9-4). With progressive age, there will be gradual fibrosis (Fig. 9-4C).
Thus, melanocytic nevi undergo the evolution from junctional → compound → dermal MN (Fig. 9-1B). Since the capacity of nevus cells to form melanin is greatest when they are located at the dermal–epidermal junction and lose their capacity for melanization the further they penetrate into the dermis, the lesser is the intensity of pigmentation with the increase in the dermal proportion of the
nevus. Purely dermal melanocytic nevi are therefore almost always without pigment. In a simplified manner, the clinical appearance of melanocytic nevi along this evolutionary path can be characterized as follows: junctional melanocytic nevus is flat and dark, compound melanocytic nevus is raised and dark, and dermal melanocytic nevus is raised and light. This evolution also reflects the age at which these lesions are found. Junctional and compound melanocytic nevi are usually seen in childhood and through the teens, whereas dermal melanocytic nevi start manifesting in the third and fourth decade.
A
B
Junctional Melanocytic Nevi
LESIONS Macule, or only very slightly raised (Fig. 9-2). Uniform tan, brown, dark brown, or even black. Round or oval with smooth, regular borders. Scattered discrete lesions. Small (≤6 mm) (see Section 12).
Compound Melanocytic Nevi
LESIONS Papules (≤6 mm) (Fig. 9-3). Dark brown, sometimes even black; dome-shaped, smooth, or cobblestone-like surface, regular and sharply defined border, sometimes papillomatous or hyperkeratotic. Consistency either firm or soft. Color may become mottled as progressive conversion into dermal melanocytic nevi occurs. May have hairs.
Dermal Melanocytic Nevi
LESIONS Sharply defined papule. Skin colored, tan, or flecks of brown, often with telangiectasia. Round, dome-shaped (Fig. 9-4), smooth surface. Usually not present before the second or third decade. Older lesions, mostly on the trunk, may become
pedunculated and do not disappear spontaneously. May be hairy. DISTRIBUTION Face, trunk, extremities, scalp. Random. Occasionally acral.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
DIAGNOSIS Made clinically. As for all pigmented lesions, the ABCDE rule applies (see Section 12). In case of doubt, apply dermoscopy, and if malignancy cannot be excluded even by this procedure, biopsy lesions with a narrow margin. DIFFERENTIAL DIAGNOSIS Junctional melanocytic nevi: All flat, deeply pigmented lesions. Solar lentigo, flat atypical nevus, and lentigo maligna. Compound melanocytic nevi: All raised pigmented lesions. Seborrheic keratosis, dysplastic nevi, melanoma, pigmented basal cell carcinoma (BCC), dermatofibroma, Spitz nevus, and blue nevus. Dermal melanocytic nevi: All light tan or skin-colored papules. BCC, neurofibroma, trichoepithelioma, dermatofibroma, and sebaceous hyperplasia.
A
B C
MANAGEMENT
Indications for removal of acquired melanocytic nevi are the following:
Growth: If there is a rapid change in size. Color: If color becomes variegated. Border: If irregular borders are present or develop. Erosions: If lesion becomes eroded without major trauma.
Symptoms: If lesion begins to persistently itch, hurt, or bleed. Dermoscopy: If criteria for melanoma or a dysplastic nevus are present or appear de novo.
If there is an indication for the removal, the nevus should preferably be excised with narrow margins for accurate histologic diagnosis.
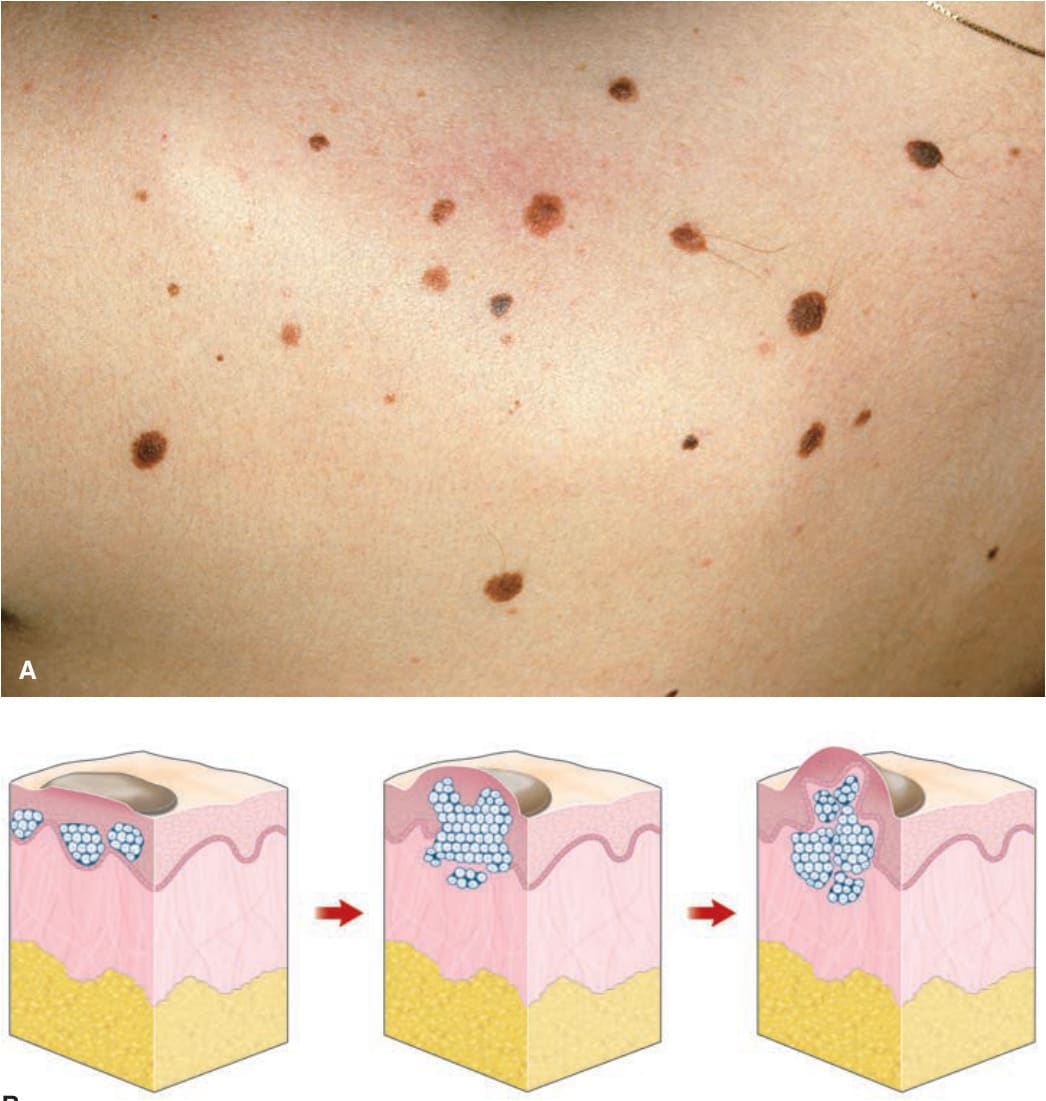
FIGURE 9-1 • (A) Multiple MN on the shoulder of a 32-year-old female Most of these nevi are junctional MN; some are slightly elevated and thus compound MN. Note relatively uniform shape and color of the lesions. Because of different developmental stages, they are of varying size ranging from 1 to 4 mm in diameter. They are regular and have a relatively uniform shape. (B) Junctional MN arise at dermal–epidermal junction and are intraepidermal, pigmented, and flat. In compound MN, nevus cells have invaded the dermis and are thus both intraepidermal and dermal. Since, as a rule, only junctional nevus cells have the capacity to form melanin, they are still pigmented, but since they continue to grow, they are more elevated than junctional MN. In dermal MN, all nevus cells are now in the dermis and have lost the capacity to produce melanin. Dermal MN are thus skin-colored, pink, or only slightly tan. As they still grow and expand into the dermis, they lift the lesion upward and are thus usually dome-shaped or papillomatous.
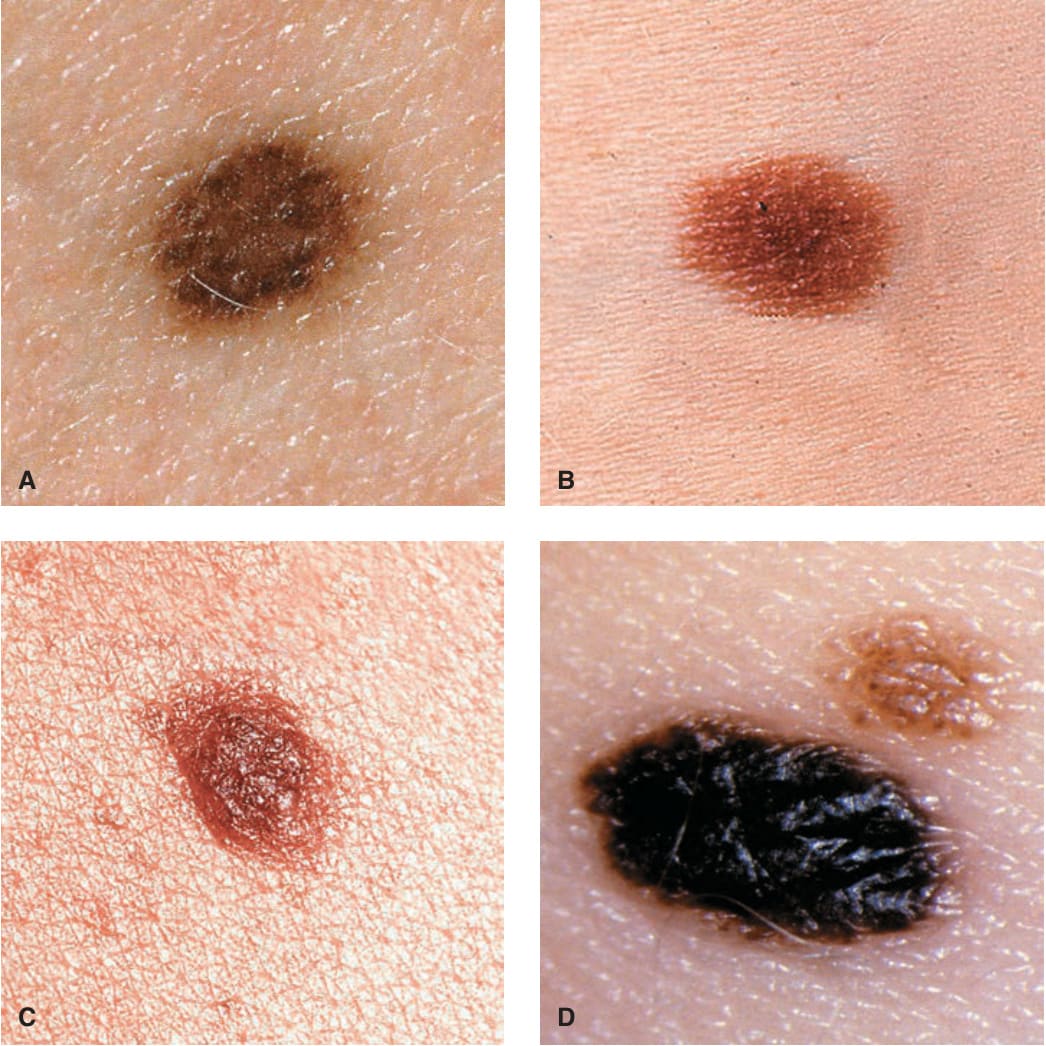
FIGURE 9-2 • (A–D) Junctional MN Lesions are completely flat (A, B) or minimally elevated as in (C) and (D). They are symmetric with a regular border and, depending on the skin type of the individuals, have different shades of brown to black (D).
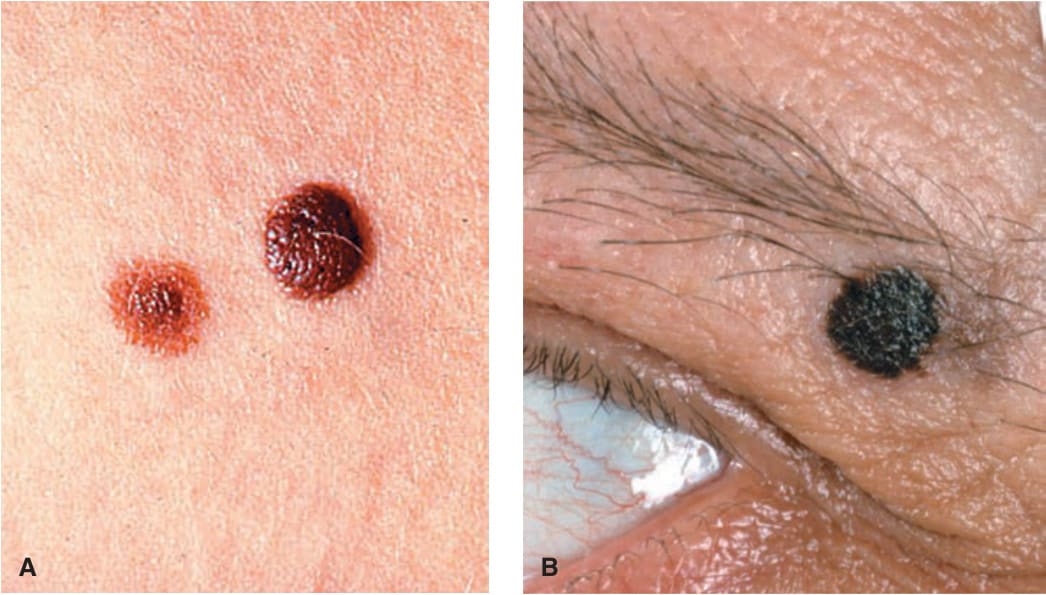
FIGURE 9-3 • Compound MN Uniformly pigmented papules and small-domed nodules. (A) The lesion to the left is flatter and tan with a more elevated darker center; the larger lesion (on the right) is older and chocolate-brown; the left lesion is younger and has a predominantly junctional component at the periphery. (B) A heavily pigmented domeshaped lesion in the eyebrow. It is sharply defined, uniformly black, smooth and slightly cobblestone-like surface, and sharply and regularly defined. It measures less than 5 mm.

FIGURE 9-4 • Dermal melanocytic MN (A) Two dome-shaped, sharply defined, relatively soft tan nodules on the left cheek and right lateral mandibular region in a 60-year-old male. These lesions were previously much darker and less elevated. (B) A larger magnification of a dermal MN. This lesion is sharply defined, has a reddish color with a central regular pigmented spot where the nevus obviously is still compound in nature. (C) Old dermal nevus on the upper lip of a 65-year-old woman. This lesion is relatively hard, has a smooth surface, and a pinkish color. This lesion is fibrosing.