HEMANGIOMA OF INFANCY (HI)
HEMANGIOMA OF INFANCY (HI) ICD-10: D18.008
Formerly strawberry, cherry, capillary hemangioma.
EPIDEMIOLOGY
The most common tumor of infancy. Incidence in newborns is between 1% and 2.5%; in Caucasian children by 1 year of age, it is 10%. Females to males ratio is 3:1.
ETIOLOGY AND PATHOGENESIS
Hemangioma of infancy (HI) is a localized proliferative process of angioblastic mesenchyme. A clonal expansion of endothelial cells resulting from somatic mutations of genes regulating endothelial cell proliferation.
CLINICAL MANIFESTATION
The initial proliferative phase lasts from 3 to 9 months. HIs usually enlarge rapidly during the first year. In a subsequent phase of involution, the HI regresses gradually over 2 to 6 years. Involution is usually completed by the age of 10 and varies greatly between individuals. It is not correlated with size, location, or appearance of the lesion. SKIN LESIONS Soft, bright red to deep purple, compressible. On diascopy, does not blanch completely. Nodule or plaque, 1 to 8 cm (Figs. 9-13A and 9-14A). With the onset of
spontaneous regression, a white-to-gray area appears on the surface of the central part of the lesion (Fig. 9-14A). Ulceration may occur.
Distribution Lesions are usually solitary and localized or extended over an entire region (Fig. 9-15). They usually cover 50% of the head and neck and 25% of the trunk. Face, trunk, legs, and oral mucous membrane.
SPECIAL PRESENTATIONS
DEEP HI (Formerly, cavernous hemangioma.) In the lower dermis and subcutaneous fat. Localized, firm rubbery mass of bluish or normal skin color with telangiectasias in overlying skin (Fig. 9-16). Can be combined with superficial hemangioma (Fig. 9-14A). Does not involute as well as superficial type. MULTIPLE HIs >5 lesions are associated with visceral involvement. CONGENITAL HEMANGIOMAS These develop in utero and are subdivided into rapidly involuting congenital hemangiomas (RICH) and noninvoluting congenital hemangiomas (NICH). They present as violaceous tumors with overlying telangiectasia with large veins
A B
A B
in periphery or as red-violaceous plaques invading deeper tissues. NICH are fast-flow hemangiomas requiring surgery.
LABORATORY EXAMINATION
DERMATOPATHOLOGY Proliferation of endothelial cells in various amounts in the dermis and/ or subcutaneous tissue; there is usually more endothelial proliferation in the superficial type and little in the deep angiomas. GLUT-1 immunoreactivity is found in all hemangiomas but not in vascular malformations.
DIAGNOSIS
Made on clinical findings and MRI; Doppler and arteriography to demonstrate fast flow. Determine GLUT-1 immunoreactivity to rule out vascular malformation.
COURSE AND PROGNOSIS
∼90% of HIs spontaneously involute by the fourth year, without much improvement seen afterwards (Figs. 9-13B and 9-14B). Residual skin changes are seen with half of the lesions—atrophy, depigmentation, telangiectasia, and scarring. HIs may, however, pose a considerable problem during the growth
phase when they interfere with vital functions, such as obstruction of vision (Fig. 9-15) or of larynx, nose, (Fig. 9-16) or mouth. Deeper lesions, especially those involving mucous membranes, may not involute completely. Synovial involvement may be associated with hemophilia-like arthropathy. Special forms of HI, tufted angiomas, and Kaposiform hemangioendothelioma, may have platelet entrapment, thrombocytopenia (Kasabach–Merritt syndrome), and even disseminated intravascular coagulation. Rarely, morbidity associated with HI occurs secondary to hemorrhage or high-output heart failure.
MANAGEMENT
Each lesion must be judged individually regarding the decision to treat or not to treat and the selection of a treatment mode. Surgical and medical interventions include continuous wave or pulsed dye laser, cryosurgery, intralesional and systemic high-dose glucocorticoids, interferon-α (IFN-α), and propranolol (Figs. 9-13B and 9-14B). Treatment is recommended for lesions that ulcerated or obstruct vital structures (eyes, ears, larynx).
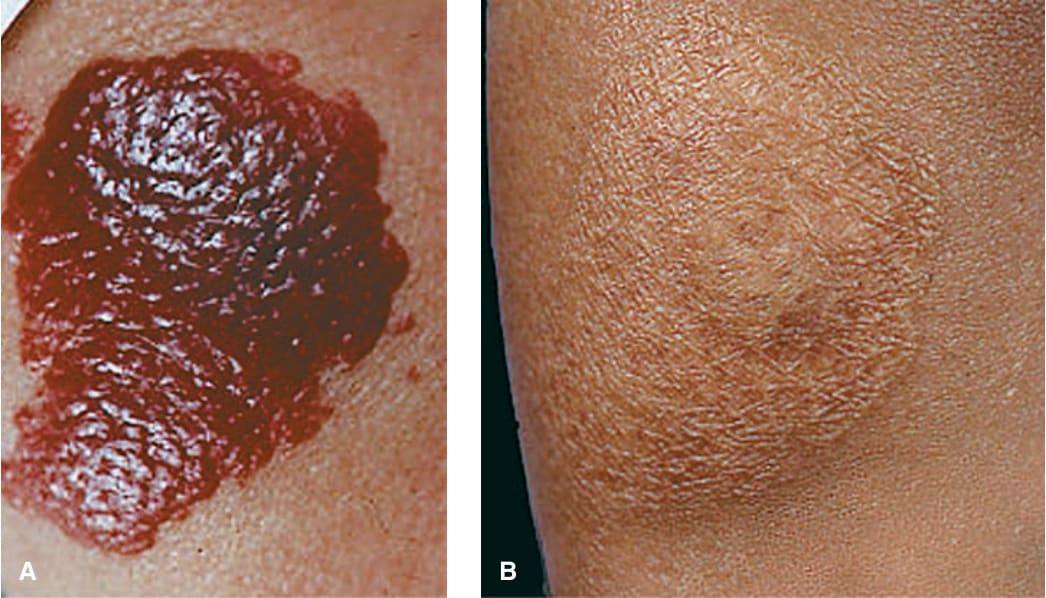
FIGURE 9-13 • Hemangioma of infancy (A) This bright red nodular plaque in an infant of African extraction is frightening to the parents, and caution is needed to prevent scarring from the treatment itself. Since most of these lesions disappear spontaneously with only 20% showing residual atrophy or depigmentation, a wait-and-see strategy is recommended. (B) The same lesion after 3 years. The hemangioma has faded spontaneously, and there is only slight residual atrophy.

FIGURE 9-14 • Hemangioma of infancy (A) This lesion on the nose consists of a superficial and deep portion, and incipient involution is already apparent for the superficial compartment. Note an additional small hemangioma of infancy on the left zygomatic region. (B) By the fifth year, the hemangioma on the nose has almost disappeared and so has the lesion on the zygomatic region; the latter, however, has left a small scar.
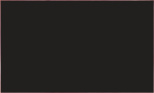
FIGURE 9-15 • Hemangioma of infancy Here, it involves a large segment of skin. While early involution is already apparent on the forehead, the lesion on the upper eyelid and the medial canthus impairs proper function of the lid, and this indicates that vision might be compromised in the future. In this patient, treatment was indicated.
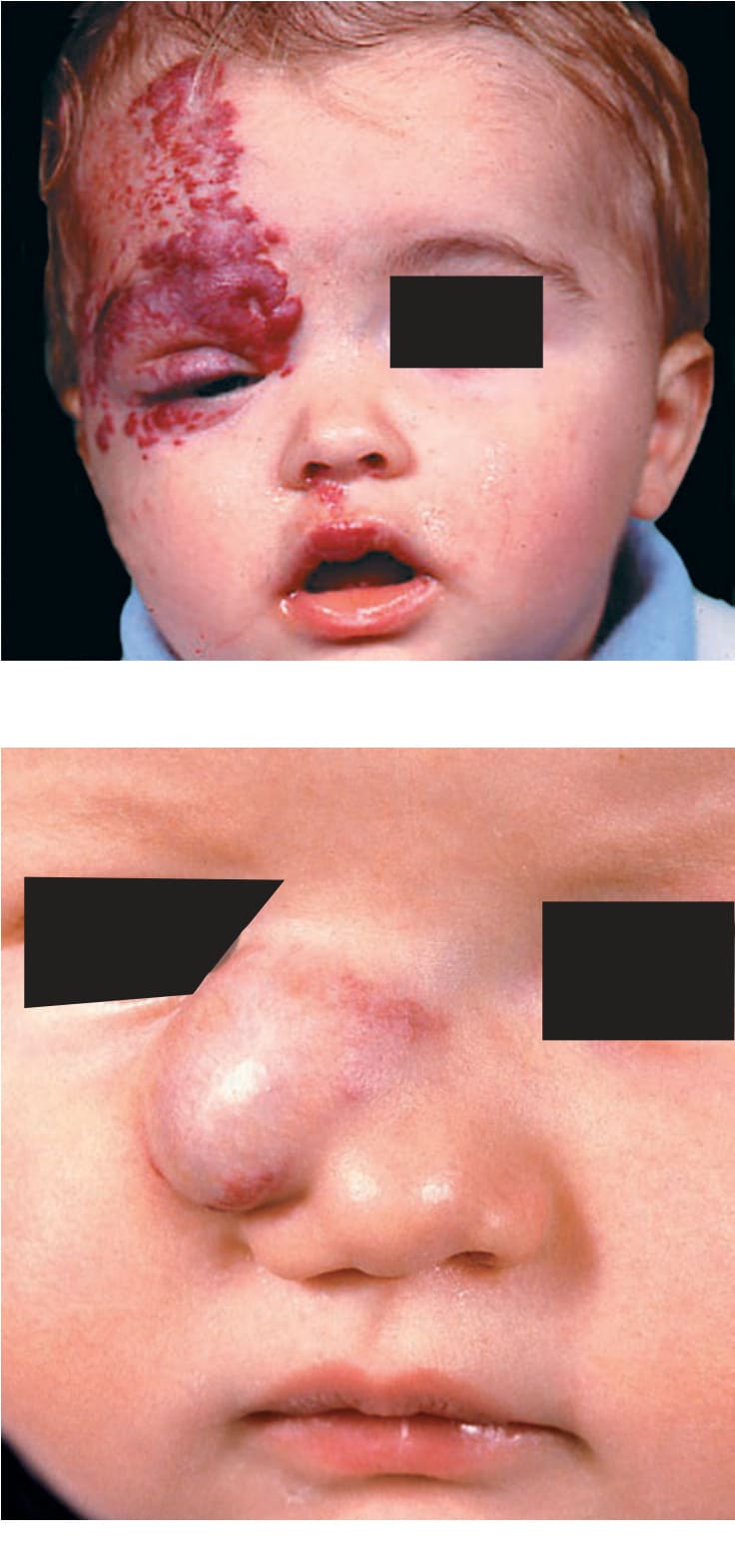
FIGURE 9-16 • Hemangioma of infancy, deep lesion There is a rubbery mass in the subcutis associated with a superficial (red) portion. These lesions hardly regress. The hemangioma was removed by surgery.