SEBORRHEIC KERATOSIS
SEBORRHEIC KERATOSIS ICD-10: L82
• The seborrheic keratosis is the most common of the benign epithelial tumors.
• These lesions, which are hereditary, do not appear until age 30 and continue to occur over a lifetime, varying in extent from a few scattered lesions to literally hundreds in some very elderly patients.
• Lesions range from small, barely elevated papules to plaques with a warty surface and a “stuck on” appearance.
• Lesions are benign and do not require treatment except for cosmetic reasons. They can become irritated or traumatized, with pain and bleeding. SCC and melanoma should be ruled out.
EPIDEMIOLOGY
ONSET Rarely before 30 years. SEX Slightly more common and more extensive involvement in males.
CLINICAL MANIFESTATION
Evolve over months to years. Rarely pruritic; tender if secondarily infected. SKIN LESIONS Early Small papule (Figs. 9-36 and 9-37) with or without pigment.
Late Plaque with warty surface and “stuck on” appearance (Fig. 9-38), “greasy.” With dermoscopy, “horn cysts” can easily be seen and are diagnostic. Brown, gray, black, skin-colored, white (Figs. 9-37 and 9-38A, B).
Distribution Isolated lesion or generalized. Face, trunk (Fig. 9-39), upper extremities. In females, commonly occur in submammary intertriginous skin. In darker-skinned people, multiple, small, black lesions in the face are called dermatosis papulosa nigra (Fig. 9-37).
LABORATORY EXAMINATION
DERMATOPATHOLOGY Proliferation of keratinocytes (with marked papillomatosis) and melanocytes, and formation of horn cysts.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Clinically, the diagnosis is made easily. “TAN MACULES” Early “flat” lesions may be confused with solar lentigo or spreading pigmented actinic keratosis (see Figs. 10-22 and 11-13). SKIN-COLORED/TAN/BLACK VERRUCOUS PAPULES/ PLAQUES Larger pigmented lesions are easily mistaken for pigmented BCC or malignant melanoma (Fig. 9-38) (only biopsy will settle this, or dermoscopy will be of assistance); verruca vulgaris may be similar in clinical appearance, but thrombosed capillaries are present in verrucae.
COURSE AND PROGNOSIS
Lesions develop with increasing age; they are benign and do not become malignant.
MANAGEMENT
Light electrocautery permits the whole lesion to be easily rubbed off. However, this precludes histopathologic verification of diagnosis and should be done only by an experienced diagnostician. Cryosurgery with liquid nitrogen spray and curettage are other treatment options.
A B

FIGURE 9-36 • Seborrheic keratosis, solitary A slightly raised, keratotic, brown, flat plaque on the zygomatic region in an older female. The differential diagnosis includes lentigo maligna and lentigo maligna melanoma.

FIGURE 9-37 • Seborrheic keratoses (dermatosis papulosa nigra) This consists of a myriad of tiny black lesions, some enlarging to more than a centimeter. This is seen in Black Africans, African Americans, and deeply pigmented South East Asians.
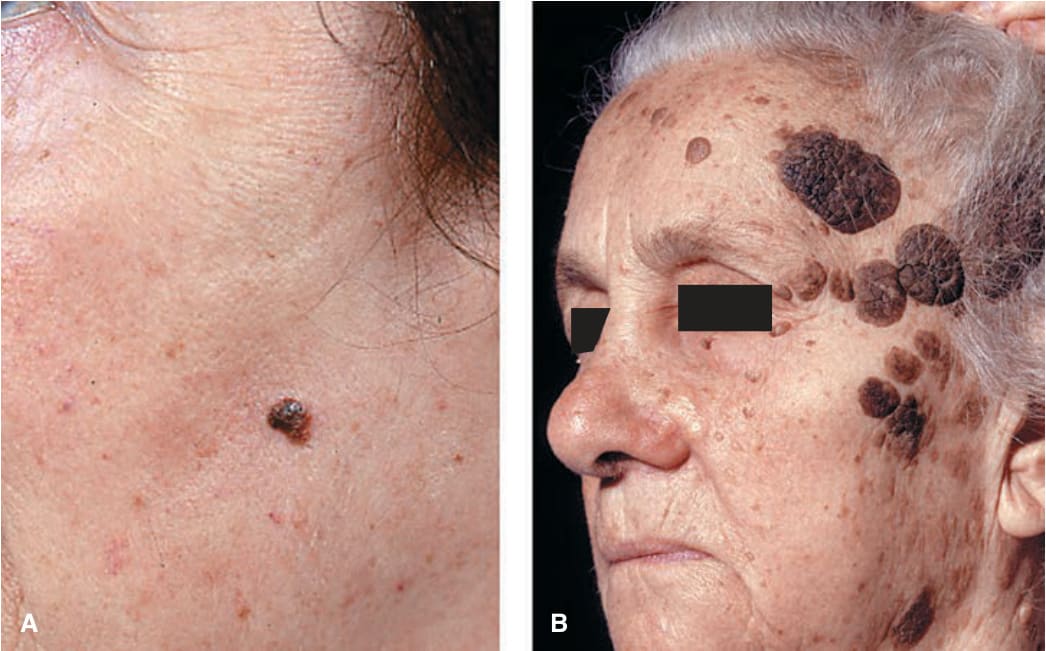
FIGURE 9-38 • Seborrheic keratosis (A) Small, heavily pigmented seborrheic keratoses can have a smooth surface and present a differential diagnostic challenge: pigmented basal cell carcinoma and nodular melanoma have to be excluded. (B) Large seborrheic keratoses have a “stuck on” appearance and can be very dark and irregular. Because of their multiplicity, they usually do not present a diagnostic problem. As shown here, they can be disfiguring.
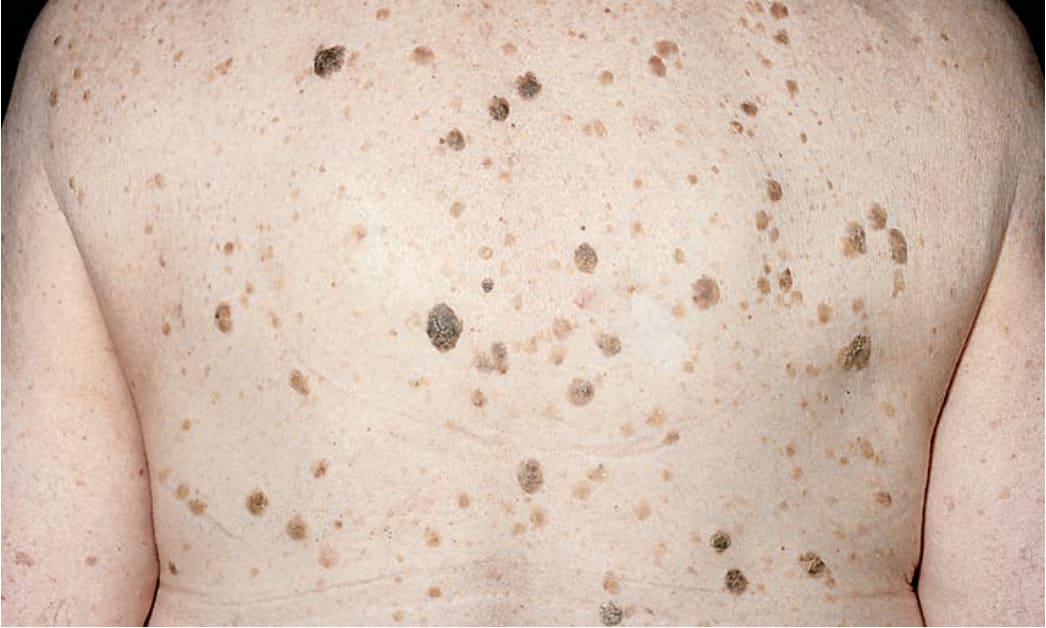
FIGURE 9-39 • Seborrheic keratoses Multiple brown, warty papules and nodules on the back, having a “greasy” feel and “stuck on” appearance. This picture also shows the evolution of the lesions: from small only slightly tan, very thin papules, or plaques to larger, darker nodular lesions with a verrucous surface. Practically all lesions on the back of this elderly patient are seborrheic keratoses; what they have in common is that they give the impression that they could be scraped off easily, which, in fact, they can.