ACTINIC KERATOSIS
ACTINIC KERATOSIS ICD-10: L57.0
• Single or multiple, discrete, dry, rough, or adherent scaly lesions on the habitually sun-exposed skin of adults, usually on a background of dermatoheliosis.
• Actinic keratoses can progress to squamous cell carcinoma.
• Synonym: Solar keratosis.
EPIDEMIOLOGY
AGE OF ONSET Middle age, although in Australia and southwestern United States, solar keratoses may occur in persons <30 years. SEX More common in males. RACE More common in light-skinned people. OCCUPATION Outdoor workers (especially farmers, ranchers, and sailors) and outdoor sportspersons (tennis, golf, mountain climbing, and deep-sea fishing).
PATHOGENESIS
Prolonged and repeated solar exposure in susceptible persons leads to cumulative damage to keratinocytes by the action of UVR, principally UVB (290 to 320 nm).
CLINICAL MANIFESTATION
SKIN SYMPTOMS Lesions may be tender. Painful if excoriated with a fingernail.
SKIN LESIONS Takes months to years to develop. Adherent hyperkeratotic scale, which is removed with difficulty and pain (Figs. 11-1 and 11-2). Rough, like coarse sandpaper, “better felt than seen” on palpation. Most commonly <1 cm, oval or round (Fig. 11-2).
Special Presentation Spreading pigmented actinic keratosis (SPAK). This lesion is best described as “looks like lentigo maligna (LM) but feels like actinic keratosis” (Fig. 11-3). Uncommon. The distinctive features of SPAK include size (>1.5 cm), pigmentation (brown to black and variegated), and history of slow spreading, especially the verrucous surface. The lesion is important because it can mimic LM.
Distribution Isolated single lesion or scattered discrete lesions. Face (forehead [Fig. 11-1], nose, cheeks, temples, vermilion border of lower lip), ears (in males), neck (sides), forearms, and hands (dorsa), shins, and the scalp in bald males (Figs. 11-1 and 11-2). Males with early pattern alopecia are especially prone to severe dermatoheliosis and solar keratosis on the exposed scalp.
LABORATORY EXAMINATION
DERMATOPATHOLOGY Large bright-staining keratinocytes, with mild-to-moderate pleomorphism in the basal layer extending into follicles, atypical (dyskeratotic) keratinocytes, and parakeratosis.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Usually made on clinical findings. Differential: Chronic cutaneous lupus erythematosus; seborrheic keratosis, flat warts, SCC (in situ), superficial BCC. Highly hyperkeratotic lesions and SPAK may require a biopsy to rule out SCC (in situ or invasive) or LM.
COURSE AND PROGNOSIS
Solar keratoses may disappear spontaneously, but in general it remains for years. The actual incidence of SCC arising in preexisting solar keratoses (Fig. 11-4) is unknown but is estimated at 1% per year.
MANAGEMENT
PREVENTION Avoided by use of highly effective UVB/UVA sunscreens.
Topical Therapy of Individual Lesions Cryosurgery. For extensive facial lesions, facial laser
resurfacing can be effective. Photodynamic Therapy. Effective but painful and cumbersome.
Topical Field Therapy This treats not only individual lesions but also inapparent early lesions. Therefore, a dermatitis results with many more
erosions than there were visible actinic keratoses. The patient has to be warned that this will occur.
5-Fluorouracil (5-FU) Cream 5%. Effective, but difficult for many individuals. Treatment of facial lesions causes significant erythema and erosions, resulting in temporary cosmetic disfigurement. Efficacy can be increased if applied under occlusion and/or combined with topical tretinoin. However, this leads to confluent erosions. Re-epithelialization occurs after treatment is discontinued.
Imiquimod (twice weekly for 16 weeks). Causes cytokine dermatitis, also leads to irritation and erosions but is highly effective.
Topical Retinoids. Used chronically, this is effective for prevention and treatment of DHe and superficial solar keratoses.
Diclofenac Gel. Used chronically, this only effective in superficial acting keratoses; also irritating.
Facial Peels. Trichloroacetic acid (5% to 10%) effective for widespread lesions.
EPITHELIAL PRECANCEROUS LESIONS AND SCCIS
Dysplasia of epidermal keratinocytes in epidermis and squamous mucosa can involve the lower portion of the epidermis or the full thickness. Basal cells mature into dysplastic keratinocytes resulting in a hyperkeratotic papule, or plaque, clinically identified as “keratosis.” A continuum exists from dysplasia to SCCIS to invasive SCC. These lesions have various associated eponyms such as Bowen disease or erythroplasia of Queyrat, which as descriptive morphologic terms are helpful; terms such as UVR- or HPV-associated SCCIS, however, would be more meaningful but can be used only for those lesions with known etiology. Epithelial precancerous lesions and SCCIS can be classified into UV-induced (solar [actinic] keratoses, lichenoid actinic keratoses, Bowenoid actinic keratoses, and Bowen disease [SCCIS]), HPV-induced (low-grade squamous intraepithelial lesions [HSIL] and Bowenoid papulosis [SCCIS]), arsenical-
induced (palmoplantar keratoses, Bowenoid arsenical) keratosis, and hydrocarbon (tar) keratoses and thermal keratoses.
SOLAR OR ACTINIC KERATOSIS (see the preceding discussion)
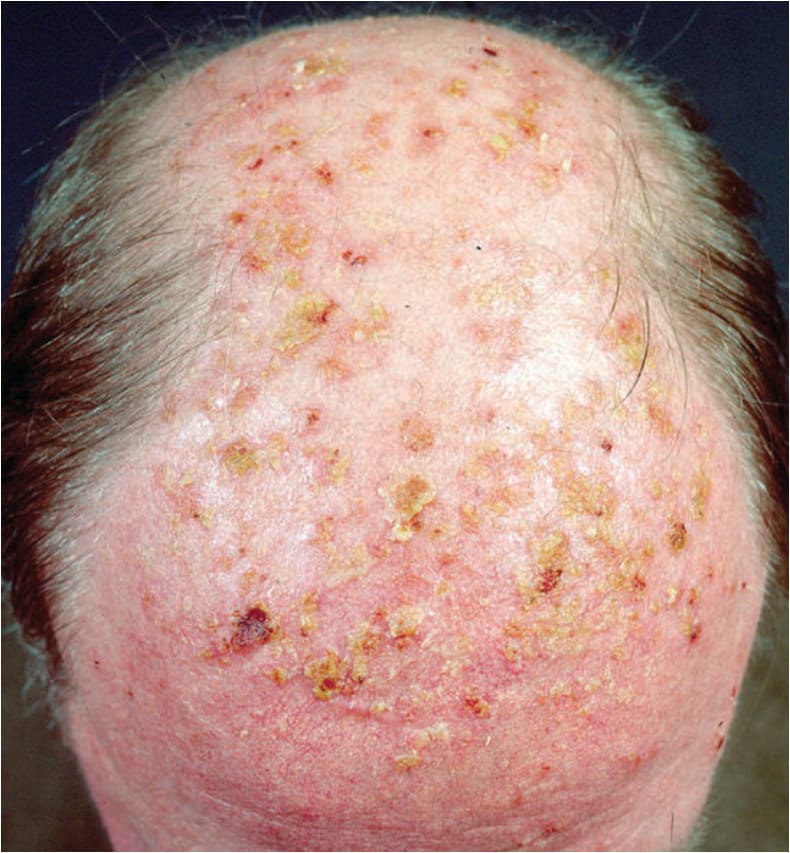
FIGURE 11-1 • Erythematous and brownish macules and papules with coarse adherent scale became confluent on the bald scalp with dermatoheliosis These hyperkeratosis are yellowish to gray. Early lesions can be better felt than seen. Gentle abrasion with the fingernail is painful, a helpful diagnostic finding.

FIGURE 11-2 • Actinic keratosis, close up. Grayish, dirty looking, tightly adherent scales Abrading these hyperkeratosis is painful and leaves erosions. There is a small BCC at the border of the hairy scalp (arrow).

FIGURE 11-3 • Spreading pigmented actinic keratosis (SPAK) “Looks like lentigo maligna (LM)” (Fig. 12-7) but “feels like actinic keratosis.”
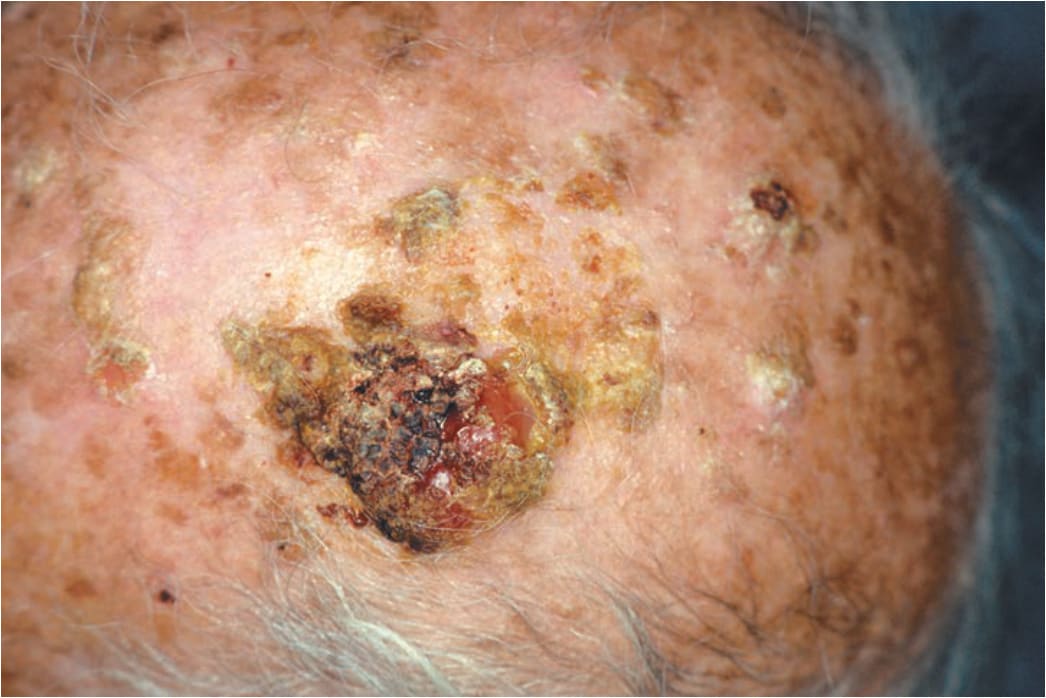
FIGURE 11-4 • Solar keratoses and invasive squamous cell carcinoma (SCC) Multiple, tightly adherent dirty looking solar keratoses. The large nodule shown here is covered by hyperkeratoses and hemorrhagic crusts; it is partially eroded and firm. This nodule is invasive squamous cell carcinoma. The image is shown to demonstrate the transition from precancerous lesions to frank carcinoma.