ARSENICAL KERATOSES
ARSENICAL KERATOSES ICD-10: L85.810
• Appear decades after chronic arsenic ingestion (medicinal, occupational, or environmental exposure). They have become very rare in industrialized countries but are currently being seen in India (West Bengal) and Bangladesh where drinking water may still contain arsenic.
• Arsenical keratoses have the potential to become SCCIS or invasive SCC.
• Two types: Punctate, yellow papules on palms and soles (Fig. 11-6A); keratoses indistinguishable from actinic keratoses on the trunk and elsewhere. These are often associated with small SCCIS of the Bowen-type and hypopigmented slightly depressed macules (“raindrops in the dust”) (Fig. 11-6B).
• Treatment—as for solar keratoses.
A
B
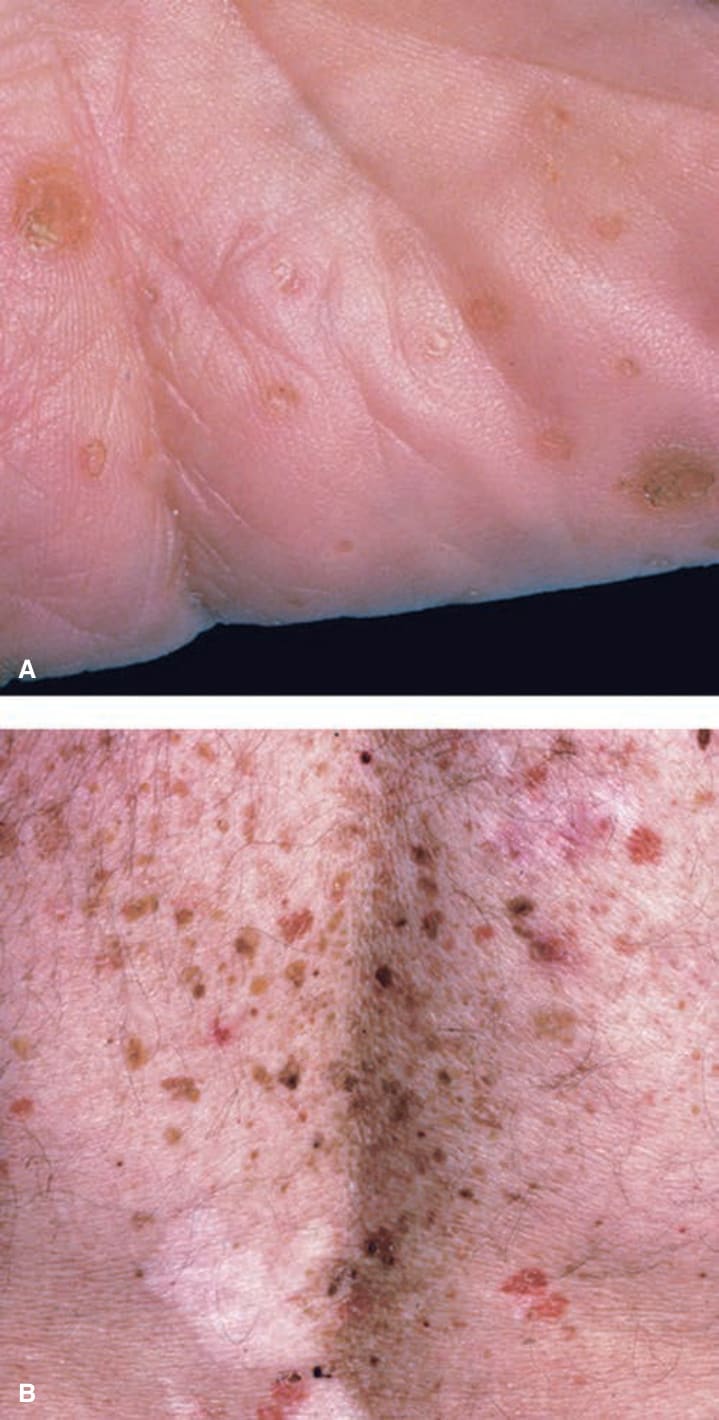
FIGURE 11-6 • Arsenical keratoses (A) Multiple punctate, tightly adherent, and very hard keratoses on the palm. (B) Arsenical keratoses on the back. Multiple lesions are seen here ranging from red to tan, dark brown, and white. The brown lesions are a mix of arsenical keratoses (hard, rough) and small seborrheic keratoses (soft and smooth). The difference can be better felt than seen. The red lesions are small Bowenoid keratoses and Bowen disease (SCCIS, see Fig. 11-7). The white macular areas are slightly depressed and represent superficial atrophic scars from spontaneously shed or treated arsenical keratoses. The entire picture gives the impression of “rain drops in the dust.”