VITILIGO
VITILIGO ICD-10: L80
• Worldwide occurrence; 1% of population affected.
• A major psychological problem for brown or black persons, resulting in severe difficulties in social adjustment.
• A chronic disorder with multifactional predisposition and triggering factors.
• Clinically characterized by totally white macules, which enlarge and can affect the entire skin.
• Microscopically: complete absence of melanocytes.
• Rarely associated with systemic autoimmune and/or endocrine disease.
EPIDEMIOLOGY
SEX Equal in both sexes. The predominance in women suggested by the literature likely reflects the greater concern of women about cosmetic appearance. AGE OF ONSET May begin at any age, but in 50% of cases it begins between the ages of 10 and 30 years. INCIDENCE Common worldwide. Affects up to 1% of the population. RACE All races. The apparently increased prevalence reported in some countries and among darker-skinned persons results from a dramatic contrast between white vitiligo macules and dark skin and from marked social stigma in countries such as India. INHERITANCE Vitiligo has a genetic background; >30% of affected individuals have reported vitiligo in a parent, sibling, or child. Vitiligo in identical twins has also been reported. Transmission is most likely polygenic with variable expression. The risk of vitiligo for children of affected individuals is unknown but may be <10%. Individuals from families with an increased prevalence of thyroid disease, diabetes mellitus, alopecia areata, and vitiligo appear to be at increased risk for development of vitiligo.
PATHOGENESIS
Three principal theories have been presented about the mechanism of destruction of melanocytes in vitiligo:
-
The autoimmune theory holds that selected melanocytes are destroyed by cytotoxic lymphocytes that have somehow been activated.
-
The self-destruct hypothesis suggests that melanocytes are destroyed by toxic substances formed as part of normal melanin biosynthesis. This could then activate mechanisms mentioned in the autoimmune hypothesis.
-
The neurogenic hypothesis is based on an interaction of the melanocytes and nerve cells. This probably holds only for segmental vitiligo.
CLINICAL MANIFESTATION
Many patients attribute the onset of their vitiligo to physical trauma (where vitiligo appears at the site of trauma—Koebner phenomenon), illness, or emotional stress. Vitiligo also appears after occupational exposure to phenolic compounds, most often 4-tertiary butyl phenol. A sunburn reaction may precipitate vitiligo. SKIN LESIONS Macules, 5 mm to 5 cm or more in diameter (Figs. 13-1 and 13-2). “Chalk” or pale white, sharply marginated. The disease progresses by gradual enlargement of the old macules or by development of new ones. Margins are convex. Trichrome vitiligo (three colors: white, light brown, and dark brown) represents different stages in the evolution of vitiligo. Pigmentation around a hair follicle in a white macule represents residual pigmentation or return of pigmentation.
Distribution Two general patterns. The focal type is characterized by one or several macules in a single site; this may be an early evolutionary stage of one of the other types in some cases. Generalized vitiligo is more common and is characterized by widespread distribution of depigmented macules, often in
a remarkable symmetry (Fig. 13-2). Typical macules occur around the eyes (Fig. 13-1) and mouth, and on digits, elbows, and knees, as well as on the low back and in genital areas (Fig. 13-3). The “lip-tip” pattern involves the skin around the mouth as well as on distal fingers and toes; lips, nipples, genitalia, and anus may be involved. Confluence of vitiligo results in large white areas, and extensive generalized vitiligo may leave only a few normally pigmented areas of skin—vitiligo universalis (Fig. 13-4). SEGMENTAL VITILIGO This is a special subset that usually develops in one unilateral region; usually does not extend beyond that initial one-sided region (though not always). Once
present, is very stable. It may have a different pathogenesis than generalized vitiligo but can be associated with vitiligo elsewhere. ASSOCIATED CUTANEOUS FINDINGS White hair and prematurely gray hair. Circumscribed areas of white hair, analogous to vitiligo macules, are called poliosis. Alopecia areata (see Section 31) and halo nevi (see Section 9). In older patients, photoaging as well as solar keratoses may occur in vitiligo macules in those with history of long exposures to sunlight but squamous cell carcinoma, limited to the white macules, is very rare. GENERAL EXAMINATION Rarely associated with thyroid disease, Hashimoto thyroiditis (Graves disease); also diabetes mellitus—probably
<5%; pernicious anemia (uncommon, but increased risk); Addison disease (very uncommon); and multiple endocrinopathy syndrome (rare). Ophthalmologic examination may reveal evidence of healed chorioretinitis or iritis. Vision is unaffected. Hearing is normal. The Vogt–Koyanagi–Harada syndrome is
Hypomelanosis of hair
vitiligo + poliosis + uveitis + dysacusis + alopecia areata.
LABORATORY EXAMINATIONS
WOOD LAMP EXAMINATION For identification of vitiligo macules in very light skin. DERMATOPATHOLOGY In certain difficult cases, a skin biopsy may be required. Vitiligo macules show normal skin except for an absence of melanocytes. ELECTRON MICROSCOPY Absence of melanocytes and of melanosomes in keratinocytes. LABORATORY STUDIES To rule out associated endocrine or autoimmune diseases.
DIAGNOSIS
Normally, diagnosis of vitiligo can be made readily on clinical examination of a patient with progressive, acquired, chalk-white, bilateral (usually symmetric), sharply defined macules in typical sites.
DIFFERENTIAL DIAGNOSIS OF VITILIGO
• Pityriasis alba (slight scaling, fuzzy margins, off-white color) (see Pityriasis alba, p. 310).
• Pityriasis versicolor alba (fine scales with greenish-yellow fluorescence under Wood lamp, positive KOH (see Pityriasis versicolor, p. 307 and Section 26).
• Leprosy (endemic areas, off-white color, usually ill-defined anesthetic macules) (see Section 25).
• Postinflammatory leukoderma (off-white macules; usually a history of psoriasis or eczema in the same macular area) (see Postinflammatory hypomelanosis [psoriasis], p. 308).
• Mycosis fungoides (may be confusing as only depigmentation may be present and biopsy is necessary) (see Postinflammatory hypopigmentation, p. 310 and Section 21).
• Chemical leukoderma (history of exposure to certain phenolic compounds). This is a difficult differential diagnosis, as melanocytes are absent as in vitiligo. It most probably is vitiligo.
• Nevus anemicus (does not enhance with Wood lamp; does not show erythema after rubbing).
• Nevus depigmentosus (stable, congenital, off-white macules, and unilateral).
• Hypomelanosis of Ito (bilateral, Blaschko lines, marble cake pattern; 60% to 75% have systemic involvement—central nervous system, eyes, and musculoskeletal system).
• Tuberous sclerosis (stable, congenital offwhite macules polygonal, ash-leaf shape, occasional segmental macules, and confetti macules) (see Section 16).
• Leukoderma associated with melanoma (is probably also vitiligo).
• Vogt–Koyanagi–Harada syndrome (vision pro blems, photophobia, and bilateral dysacusis).
• Waardenburg syndrome (commonest cause of congenital deafness, white macules and white forelock, and iris heterochromia).
• Piebaldism (congenital, white forelock, stable, dorsal pigmented stripe on back,
and distinctive pattern with large hyperpigmented macules in the center of the hypomelanotic areas).
COURSE AND PROGNOSIS
Vitiligo is a chronic disease. The course is highly variable, but rapid onset followed by a period of stability or slow progression is most characteristic. Up to 30% of patients may report some spontaneous repigmentation in a few areas, particularly areas that are exposed to the sun. Rapidly progressive, or “galloping,” vitiligo may quickly lead to extensive depigmentation with a total loss of pigment in skin and hair, but not eyes. The treatment of vitiligo-associated disease (i.e., thyroid disease) has no impact on the course of vitiligo.
MANAGEMENT
The approaches to the management of vitiligo are as follows:
Sunscreens The dual objectives of sunscreens are protection of involved skin from acute sunburn
reaction and limitation of tanning of normally pigmented skin.
Cosmetic Coverup The objective of coverup with dyes or makeup is to hide the white macules so that the vitiligo is not apparent.
Repigmentation The objective of repigmentation (Figs. 13-5 and 13-6) is the permanent return of normal melanin pigmentation. LOCALIZED MACULES
• Topical glucocorticoids: Monitor for signs of early steroid atrophy.
• Topical calcineurin inhibitors: Tacrolimus and pimecrolimus. They are reported to be most effective when combined with UVB or excimer laser therapy.
• Topical photochemotherapy: topical 8-methoxypsoralen (8-MOP) and UVA.
• Excimer laser (308 nm): Best results in the face.
GENERALIZED VITILIGO
• Systemic photochemotherapy: Oral PUVA may be done with sunlight or artificial UVA
and either 5-MOP (available in Europe) or 8-MOP. Is up to 85% effective in >70% of patients with vitiligo of the head, neck, upper arms and legs, and trunk (Figs. 13-5 and 13-6). However, at least 1 year of treatment is required to achieve this result. Distal hands and feet, and the “lip-tip” variant of vitiligo are only poorly responsive.
• Narrow-band UVB, 312 nm: This is just as effective as PUVA and does not require psoralens. It is the treatment of choice in children <6 years of age.
Note: Response to all treatments is slow. When it occurs, it is signaled by tiny, usually follicular macules of pigmentation (Fig. 13-5).
Minigrafting Minigrafting (autologous Thiersch grafts, suction blister grafts, autologous minipunch
grafts, and transplantation of cultured autologous melanocytes) may be a useful technique for refractory and stable segmental vitiligo macules. “Pebbling” of the grafted site may occur.
Depigmentation The objective of depigmentation is “one” skin color in patients with extensive vitiligo or in those who have failed or reject other treatments. TREATMENTS Bleaching of normally pigmented skin with monobenzylether of hydroquinone 20% (MEH) cream is a permanent, irreversible process. The success rate is >90%. The end-stage color of depigmentation with MEH is chalk-white, as in vitiligo macules.

FIGURE 13-1 • Vitiligo: face Extensive depigmentation of the central face. Involved vitiliginous skin has convex borders, extending into the normal pigmented skin. Note the chalk-white color and sharp margination. Note also that the dermal melanocytic nevus on the upper lip has retained its pigmentation.

FIGURE 13-2 • Vitiligo: knees Depigmented, sharply demarcated macules on the knees. Apart from the loss of pigment, vitiliginous skin appears normal. There is striking symmetry. Note tiny follicular pigmented spots within the vitiligo areas that represent repigmentation.
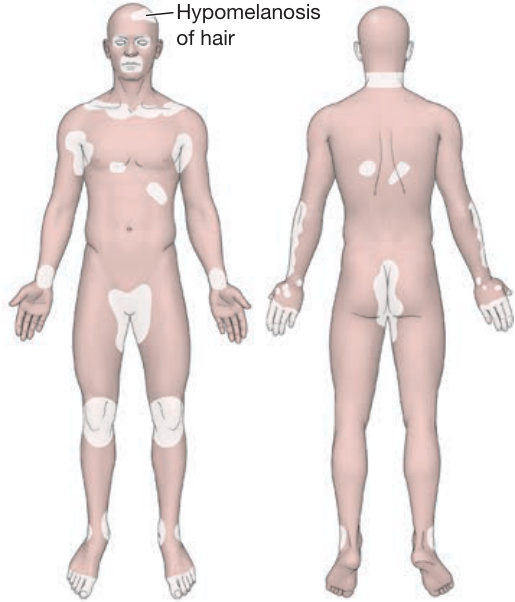
FIGURE 13-3 • Vitiligo: predilection sites.

FIGURE 13-4 • Universal vitiligo Vitiliginous macules have coalesced to involve all skin sites with complete depigmentation of skin and hair in a female. The patient is wearing a black wig and has darkened the brows with eyebrow pencil and eyelid margins with eye liner.

FIGURE 13-5 • Vitiligo repigmentation A follicular pattern of repigmentation caused by PUVA therapy occurring in a large vitiliginous macule on the lower abdomen. By confluence of the macules, the vitiliginous areas have almost filled in but are still lighter than the surrounding normal skin. Melanocytes may persist in the hair follicle epithelium and serve to repopulate involved skin, spontaneously, with photochemotherapy, or with 312 nm phototherapy.

FIGURE 13-6 • Vitiligo: therapy-induced repigmentation This 20-year-old Indian female has been treated with photochemotherapy (PUVA). There is slight erythema in the vitiliginous macules in the early phases (left) of therapy that will be followed by follicular pigmentation as in Figure 13-5. After 1 year of treatment, vitiligo has completely repigmented, but there is now hyperpigmentation of the knees (right). This, however, will fade with time and the color of the repigmented areas will blend with that of the surrounding skin.