HYPERPIGMENTATION
HYPERPIGMENTATION ICD-10: L81.010
• Postinflammatory epidermal melanin hyperpigmentation is a major problem for patients with skin phototypes IV, V, and VI (Figs. 13-10 and 13-11). This disfiguring pigmentation can develop with acne (Fig. 13-10), psoriasis, lichen planus (Fig. 13-11), atopic dermatitis, contact dermatitis, or after any type of trauma to the skin. It may persist for weeks to months and does not always respond to topical hydroquinone, which may accelerate its disappearance. Lesions are characteristically limited to the site of the preceding inflammation and usually have indistinct, feathered borders.
• Ashy dermatosis is a slate grey macular hyperpigmentation in skin phototype IV individuals. This is dermal hyperpigmentation and is indistinguishable from hyperpigmentation following lichen planus.
• Some drug eruptions may be associated with dermal melanin hyperpigmentation (Fig. 13-12). Dermal and epidermal hyperpigmentation may occur in macular amyloidosis (see Macular amyloidosis, Section 14).
• Riehl melanosis (melanodermatitis toxica) is a reticular, confluent black to brown- violet pigmentation of the face and neck (Fig. 13-13). It may be a result of contact sensitivity or photocontact sensitivity related to chemicals, particularly fragrance in cosmetics.
For hypermelanosis caused by phototoxic reactions induced by psoralens (Berloque dermatitis), see Section 10 and for nonmelanin-based hyperpigmentation resulting from drugs, see Section 23.
A B

FIGURE 13-10 • Hypermelanosis with acne In this 30-year-old Pakistani woman, hypermelanosis due to acne, combined with melasma and hypopigmented acne scars, was considered a cosmetic disaster, not only by the patient but also by her husband. She was successfully treated with 3% hydroquinone incorporated into a 0.05% tretinoin cream.

FIGURE 13-11 • Postinflammatory hyperpigmentation This may follow a drug eruption, or lichen planus, especially in skin phototypes IV, V, and VI, as was the case in this middle-aged East Indian man. There is a condition described as Ashy dermatosis, which is clinically indistinguishable from postinflammatory hyperpigmentation following lichen planus as shown here. Postinflammatory hyperpigmentation is a major problem in young females with skin phototypes IV and V.

FIGURE 13-12 • Postinflammatory dermal hyperpigmentation This appeared on the hand of a skin phototype IV African woman following a fixed drug eruption.
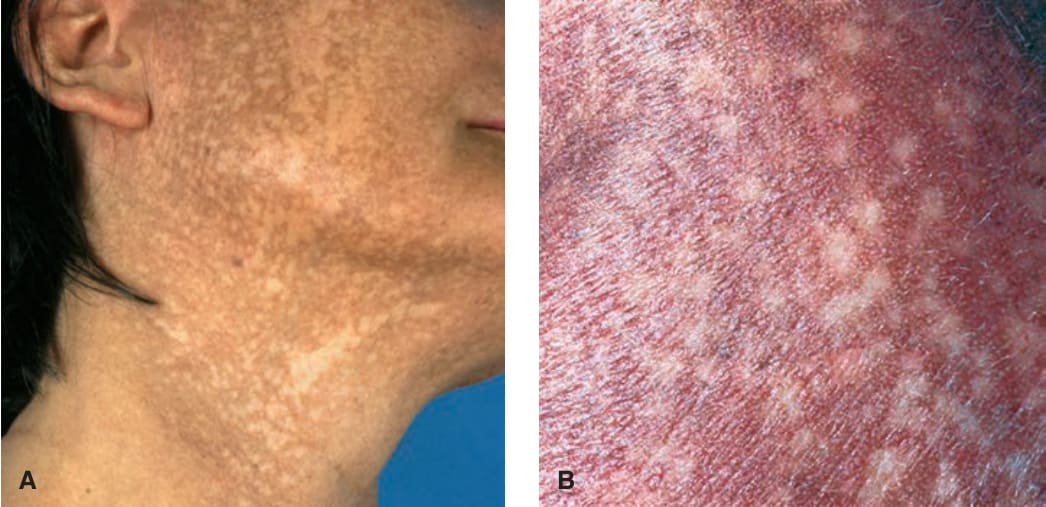
FIGURE 13-13 • Melanodermatitis toxica (A) A reticular confluent pigmentation on the face and neck of a 42-yearold female chemist who worked for a cosmetic industry and had applied, over years, most of the scented products she was involved in producing to her own skin. Since she lived in a sunny climate, this increases the suspicion of a chronic photocontact sensitivity. (B) In this Indian woman, the mottled hyperpigmentation has coalesced to dark brown mottled hyperpigmentation of the cheeks. This patient had also excessively used cosmetics for professional reasons. Such cases are not so rare in India and are called Indian lichen planus; however, the relationship to common lichen planus is not clear.