HYPOPIGMENTATION
HYPOPIGMENTATION ICD-10: L81.89
• Postinflammatory hypomelanosis is always related to loss of melanin. It is a special feature of pityriasis versicolor (Fig. 13-14, see also Section 26), in which the hypopigmentation may also remain for weeks after the active infection has disappeared.
• Hypomelanosis is not uncommonly seen in atopic dermatitis, psoriasis (Fig. 13-15), guttate parapsoriasis, and pityriasis lichenoides chronica.
• It may also be present in cutaneous lupus erythematosus (Fig. 13-16), alopecia mucinosa, mycosis fungoides (Fig. 13-17), lichen striatus, seborrheic dermatitis, and leprosy (see Hansen Disease [Leprosy], Section 25).
• Hypomelanosis may follow dermabrasion and chemical peels. In these conditions, there is a “transfer block,” in which melanosomes are present in melanocytes but are not transferred to keratinocytes, resulting in hypomelanosis. The lesions are usually not chalk-white, as in vitiligo, but “off” white and have indiscrete margins.
• A common type of hypopigmentation is associated with pityriasis alba (Fig. 13-18). This is a macular hypopigmentation mostly on the face of children, off-white with a powdery scale. Relatively indistinct margins under Wood light and scaling distinguish this eczematous dermatitis from vitiligo. It is self-limited.
• Hypomelanosis not uncommonly follows intralesional glucocorticoid injections. When the injections are stopped, a normal pigmentation develops in the areas.
• Depending on the associated disorder, postinflammatory hypomelanosis may respond to oral PUVA photochemotherapy.
A B
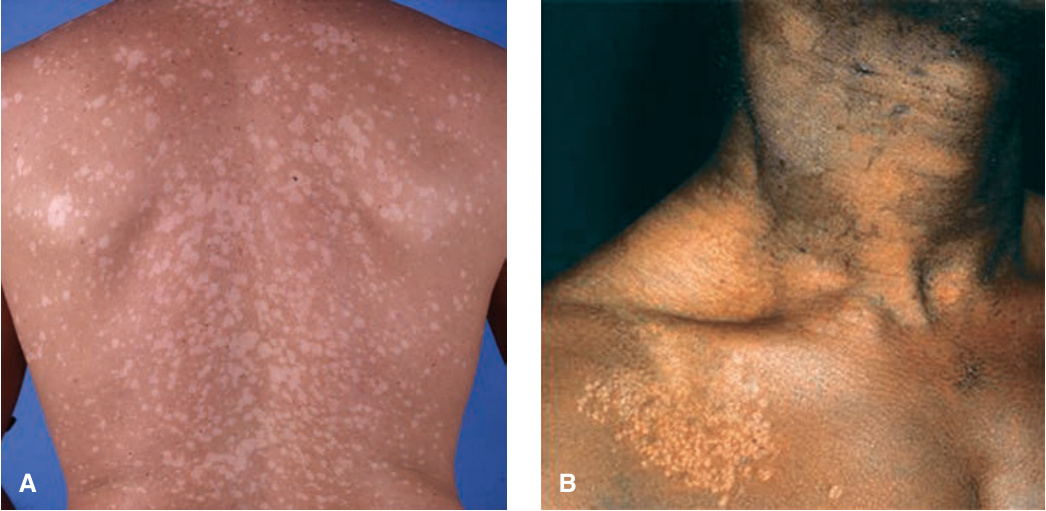
FIGURE 13-14 • Pityriasis versicolor (A) Hypopigmented, sharply marginated, scaling macules on the back of an individual with skin phototype III. Gentle abrasion of the surface will accentuate the scaling. This type of hypomelanosis can remain long after the eruption has been treated and the primary process has resolved. (B) Pityriasis versicolor in African skin Lesions are perifollicular on the chest and coalesce to large confluent patches on the neck where the fine scaling can best be seen.

FIGURE 13-15 • Postinflammatory hypomelanosis (psoriasis) The hypomelanotic lesions correspond exactly to the antecedent eruption. There is some residual psoriasis within the lesions.

FIGURE 13-16 • Postinflammatory hypopigmentation in a 33-year-old Vietnamese female. The patient had had chronic cutaneous lupus erythematosus. Residual inflammation of lupus is still seen on the upper lip.

FIGURE 13-17 • Mottled hypopigmentation, but also hyperpigmentation in mycosis fungoides. This patient had been treated with electron beam therapy.

FIGURE 13-18 • Pityriasis alba A common disfiguring hypomelanosis, which, as the name indicates, is a white area (alba) with very mild scaling (pityriasis). It is observed in a large number of children in the summer in temperate climates. It is mostly a cosmetic problem in persons with brown or black skin and commonly occurs on the face, as in this child. Among 200 patients with pityriasis alba, 90% ranged from 6 to 12 years of age. In young adults, PA quite often occurs on the arms and trunk.