SCLERODERMA
SCLERODERMA ICD-10: M34
• Scleroderma is a multisystem disorder characterized by inflammatory, vascular, and sclerotic changes of the skin and various internal organs, especially the lungs, heart, and GI tract.
• Limited systemic scleroderma (lSSc) (60%) and diffuse systemic scleroderma (dSSc) are recognized.
• Clinical features always present are skin sclerosis and Raynaud phenomenon.
• Considerable morbidity; high mortality of dSSc.
• Synonyms: Progressive systemic sclerosis, systemic sclerosis, and systemic scleroderma.
EPIDEMIOLOGY
PREVALENCE Twenty per million of the US population. AGE OF ONSET Thirty to 50 years. SEX Female:male ratio, 4:1.
CLASSIFICATION
Systemic scleroderma can be divided into two subsets: limited systemic scleroderma (lSSc) and diffuse systemic scleroderma (dSSc). lSSc patients comprise 60%; patients are usually female; older than those with dSSc; and have a long history of Raynaud phenomenon with skin involvement limited to hands, feet, face, and forearms (acrosclerosis) and a high incidence of anticentromeric antibodies. lSSc
includes the CREST syndrome, and systemic involvement may not appear for years; patients usually die of other causes. dSSc patients have a relatively rapid onset and diffuse involvement, not only of hands and feet but also of the trunk and face, synovitis, tendosynovitis, and early onset of internal involvement. Anticentromere antibodies are uncommon, but Scl-70 (antitopoisomerase I) antibodies are present in 33%.
ETIOLOGY AND PATHOGENESIS
Unknown. Primary event might be endothelial cell injury in blood vessels. Edema occurs, followed by fibrosis; cutaneous capillaries are reduced in number; remainder
dilate and proliferate, becoming visible telangiectasia.
CLINICAL MANIFESTATION
Raynaud phenomenon (see p. 352) with digital pain, coldness. Pain/stiffness of fingers and knees. Migratory polyarthritis. Heartburn, dysphagia, especially with solid foods. Constipation, diarrhea, abdominal bloating, malabsorption, and weight loss. Exertional dyspnea and dry cough. SKIN Hands/Feet Early: Raynaud phenomenon with triphasic color changes, that is, pallor, cyanosis, and rubor (Fig. 14-39B, see also Fig. 14-37). Precedes sclerosis by months and years. Nonpitting edema of hands/feet. Painful ulcerations at fingertips (“rat bite necrosis”) (Fig. 14-40A), knuckles; heal with pitted scars. Late: Sclerodactyly with tapering of fingers (Madonna fingers) (Fig. 14-39A) with waxy, shiny, hardened skin, which is tightly bound down and does not permit folding or wrinkling; leathery crepitation over joints, flexion contractures; periungual telangiectasia, nails grow clawlike over shortened distal phalanges (Fig. 14-39B). Bony resorption and ulceration results in loss of distal phalanges. Loss of sweat glands with anhidrosis; thinning and complete loss of hair on distal extremities.
Face Early: Periorbital edema. Late: Edema and fibrosis result in loss of normal facial lines, mask-like (patients look younger than they are) (Fig. 14-41), thinning of lips, microstomia, radial perioral furrowing (Fig. 14-40B), and beak-like sharp nose. Telangiectasia (Fig. 14-42) and diffuse hyperpigmentation.
Trunk In dSSc, the chest and proximal upper and lower extremities are involved early. Tense, stiff, and waxy appearing skin that cannot be folded. Impairment of respiratory movement of chest wall and of joint mobility. OTHER CHANGES Cutaneous Calcification Occurs on fingertips or over bony prominences or any sclerodermatous site; may ulcerate and exude white paste.
Color Changes Hyperpigmentation that may be generalized and on the extremities may be accompanied by perifollicular hypopigmentation.
Mucous Membranes Sclerosis of sublingual ligament; uncommonly, painful induration of gums, and tongue.
Distribution of Lesions Early: In lSSc, early involvement is seen on the fingers, hands, and face, and in many patients scleroderma remains confined to these regions. Late: The distal upper
A B
A B
and lower extremities may be involved and occasionally the trunk. In dSSc, sclerosis of the extremities and the trunk may start soon after or concomitant with acral involvement. CLINICAL VARIANT CREST syndrome, that is, calcinosis cutis +Raynaud phenomenon +esophageal dysfunction +sclerodactyly +telangiectasia. Macular, mat-like telangiectasia, especially the face (Fig. 14-42), upper trunk, and hands; also in the entire GI tract. Calcinosis over bony prominences, fingertips, elbows, and trochanteric regions.
GENERAL EXAMINATION
Esophagus Dysphagia, diminished peristalsis, and reflux esophagitis. GASTROINTESTINAL SYSTEM Small intestine involvement may produce constipation, diarrhea, bloating, and malabsorption. LUNG Pulmonary fibrosis and alveolitis. Reduction in pulmonary function resulting from restricted movement of chest wall. HEART Cardiac conduction defects, heart failure, and pericarditis. KIDNEY Renal involvement in 45%. Slowly progressive uremia, malignant hypertension.
MUSCULOSKELETAL SYSTEM Carpal tunnel syndrome. Muscle weakness.
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY Early: Mild cellular infiltrate around dermal blood vessels, eccrine coils, and at the dermal subcutaneous interphase. Late: Broadening and homogenization of collagen bundles, obliteration and decrease of interbundle spaces, thickening of dermis with replacement of upper or total subcutaneous fat by hyalinized collagen. Paucity of blood vessels, thickening/hyalinization of vessel walls. AUTOANTIBODIES Patients with dSSc have circulating ANA. Autoantibodies react with centromere proteins or DNA topoisomerase I; fewer patients have antinuclear antibodies. Anticentromeric autoantibodies occur in 21% of dSSc and 71% of CREST patients, DNA topoisomerase I (Scl-70) antibodies in 33% of dSSc and 18% of CREST patients. Anti-RNA polymerase III is associated with renal crisis and increased mortality; anti-PM-Scl with Raynaud’s and better prognosis.

FIGURE 14-37 • Raynaud phenomenon The hand exhibits a distal cyanosis; it is seen especially well in the nailbeds; proximally the skin is white resulting from vasospasm. Episodes such as this one may occur after contact with cold water.
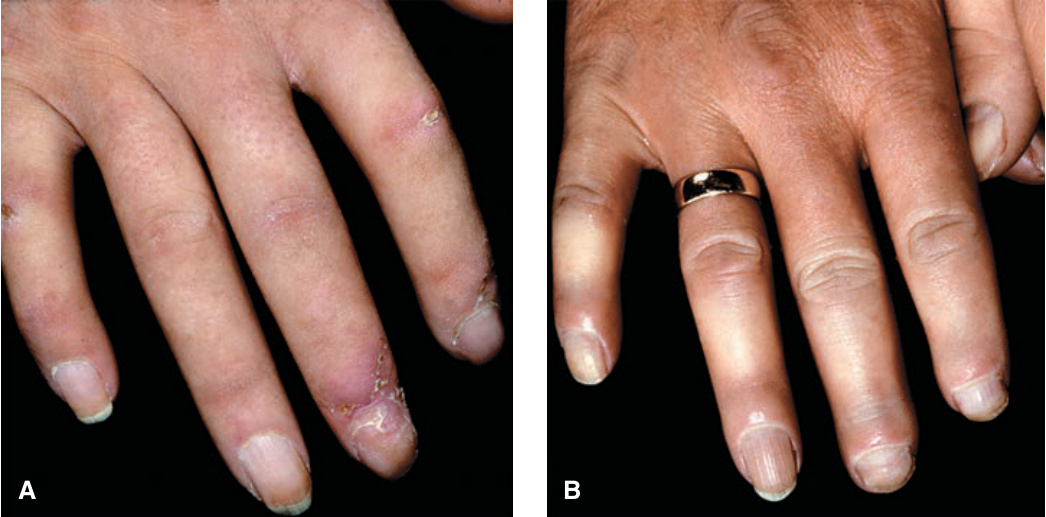
FIGURE 14-39 • Scleroderma (lSSc): acrosclerosis (A) Hands and fingers are edematous (nonpitting); skin is without skin folds and bound down. Distal fingers are tapered (Madonna fingers). (B) Fingers show both bluish erythema and vasoconstriction (blue and white): Raynaud phenomenon. Fingers are edematous, the skin is bound down. Distal phalanges (index and third finger) are shortened, which is associated with bony resorption.
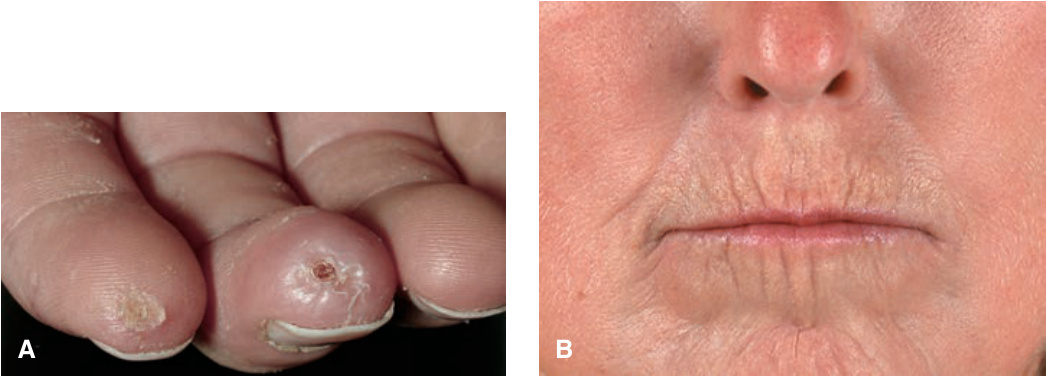
FIGURE 14-40 • Scleroderma (lSSc): acrosclerosis (A) Typical “rat bite” necroses and ulcerations of fingertips. (B) Thinning of lips—microstomia (which would show better when patient attempts to open her mouth), radial perioral furrowing. Beaklike sharp nose.

FIGURE 14-41 • Scleroderma (dSSc) Mask-like facies with stretched, shiny skin and loss of normal facial lines giving a younger appearance than actual age; the hair is dyed. Thinning of the lips and perioral sclerosis result in a small mouth. Sclerosis (whitish, glistening areas) and multiple telangiectases (not visible at this magnification) are also present.

FIGURE 14-42 • Scleroderma: CREST syndrome Numerous macular or matlike telangiectases on the forehead. (Used with permission of Dr. Kenneth Greer.)