NEUROFIBROMATOSIS (NF)
NEUROFIBROMATOSIS (NF) ICD-10: Q85.0
• NF is an autosomal-dominant trait manifested by changes in the skin, nervous system, bones, and endocrine glands. These changes include a variety of congenital abnormalities, tumors, and hamartomas.
• Two major forms of NF are recognized: (1) classic von Recklinghausen NF, termed NF1 and (2) central or acoustic NF, termed NF2. Several less common variants have also been reported (variants NF3-NF7).
• Both common types have café-au-lait macules and neurofibromas, but only NF2 has bilateral acoustic neuromas (unilateral acoustic neuromas are a variable feature of NF1).
• An important diagnostic sign present only in NF1 is pigmented hamartomas of the iris (Lisch nodules).
• Synonym: von Recklinghausen disease.
EPIDEMIOLOGY
INCIDENCE NF1: 1:4000; NF2: 1:50,000. RACE All races. SEX Males slightly more than females. HEREDITY Autosomal dominant; the gene for NF1 is on chromosome 17 (q1.2) and the gene codes for a protein named neurofibromin. The gene for NF2 is on chromosome 22 and codes for a protein called merlin.
CLINICAL MANIFESTATION
Café-au-lait (CAL) macules are not usually present at birth but appear during the first 3 years; neurofibromata appear during late adolescence. Clinical manifestations in various organs are related to pathology such as hypertensive headaches (pheochromocytomas), pathologic fractures (bone cysts), mental retardation, brain tumor (astrocytoma), short stature, and precocious puberty (early menses or clitoral hypertrophy). SKIN LESIONS CAL Macules Light or dark brown uniform melanin pigmentation with sharp margination. Lesions vary in size from multiple “freckle-like” tiny macules <2 mm (Fig. 16-6, “axillary freckling” is pathognomonic) to large brown macules >20 cm (Fig. 16-7). CAL macules also vary in number, from a few to hundreds.
Papules/Nodules (Neurofibromas) Skin-colored, pink, or brown (Fig. 16-7); flat, dome shaped or pedunculated (Fig. 16-8); soft or firm, sometimes tender; “buttonhole sign”—invagination with the tip of the index finger is pathognomonic.
Plexiform Neuromas Drooping, soft (Figs. 16-7 and 16-9), doughy; may be massive, involving entire extremity, the head, or a portion of the trunk.
Distribution Randomly distributed but may be localized to one region (segmental NF1). The segmental type may be heritable or a sporadic hamartoma. OTHER PHYSICAL FINDINGS Eyes Pigmented hamartomas of the iris (Lisch nodules) begin to appear at the age of 5 and are present in 20% of children with NF before age 6 but can be found in 95% of patients with NF1 in adolescence (Fig. 16-10). They do not correlate with the severity of the disease. They are not present in NF2.
Adrenal Pheochromocytoma Elevated blood pressure and episodic flushing.
Peripheral Nervous System Elephantiasis neuromatosa (gross disfigurement from NF of the nerve trunks).
Central Nervous System Optic glioma, acoustic neuroma (rare in NF1 and unilateral, but common and bilateral in NF2), astrocytoma, meningioma, and neurofibroma.
Hematologic Juvenile chronic myelogenous leukemia may be overrepresented.
LABORATORY EXAMINATIONS
WOOD LAMP EXAMINATION In white persons with pale skin, the CAL macules are more easily visualized with Wood lamp examination.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Two of the following criteria:
• Multiple CAL macules—more than six lesions with a diameter of 1.5 cm in adults and more than five lesions with a diameter of 0.5 cm or more in children younger than 5 years.
• Multiple freckles in the axillary and inguinal regions.
• Based on clinical and histologic grounds, two or more neurofibromas of any type, or one plexiform neurofibroma.
• Sphenoid wing dysplasia or congenital bowing or thinning of long bone cortex, with or without pseudoarthrosis.
• Bilateral optic nerve gliomas.
• Two or more Lisch nodules on slit-lamp examination.
• First-degree relative (parent, sibling, or child) with NF1 by the preceding criteria.
DIFFERENTIAL DIAGNOSIS Brown CAL-type macules: Albright syndrome (polyostotic fibroma, dysplasia, and precocious puberty); note: a few CAL macules (three or less) may be present in 10% to 20% of normal population.
COURSE AND PROGNOSIS
There is variable involvement of the organs affected over time, from only a few pigmented macules to marked disfigurement with thousands of nodules, segmental hypertrophy, and plexiform neuromas. The mortality rate is higher than in the normal population, principally because of the development of neurofibrosarcoma during adult life. Other serious complications are relatively infrequent.
MANAGEMENT
COSMETIC COUNSELING NF support groups help with social adjustment in severely affected persons. An orthopedic physician should manage the two major bone problems: kyphoscoliosis and tibial bowing. A plastic surgeon is involved in reconstructive surgery for facial asymmetry. The language disorders and learning disabilities should be evaluated by a psychologist. Close follow-up annually should be mandatory to detect sarcomas that may arise within plexiform neuromas. Support Group: http://www.nfnetwork.org
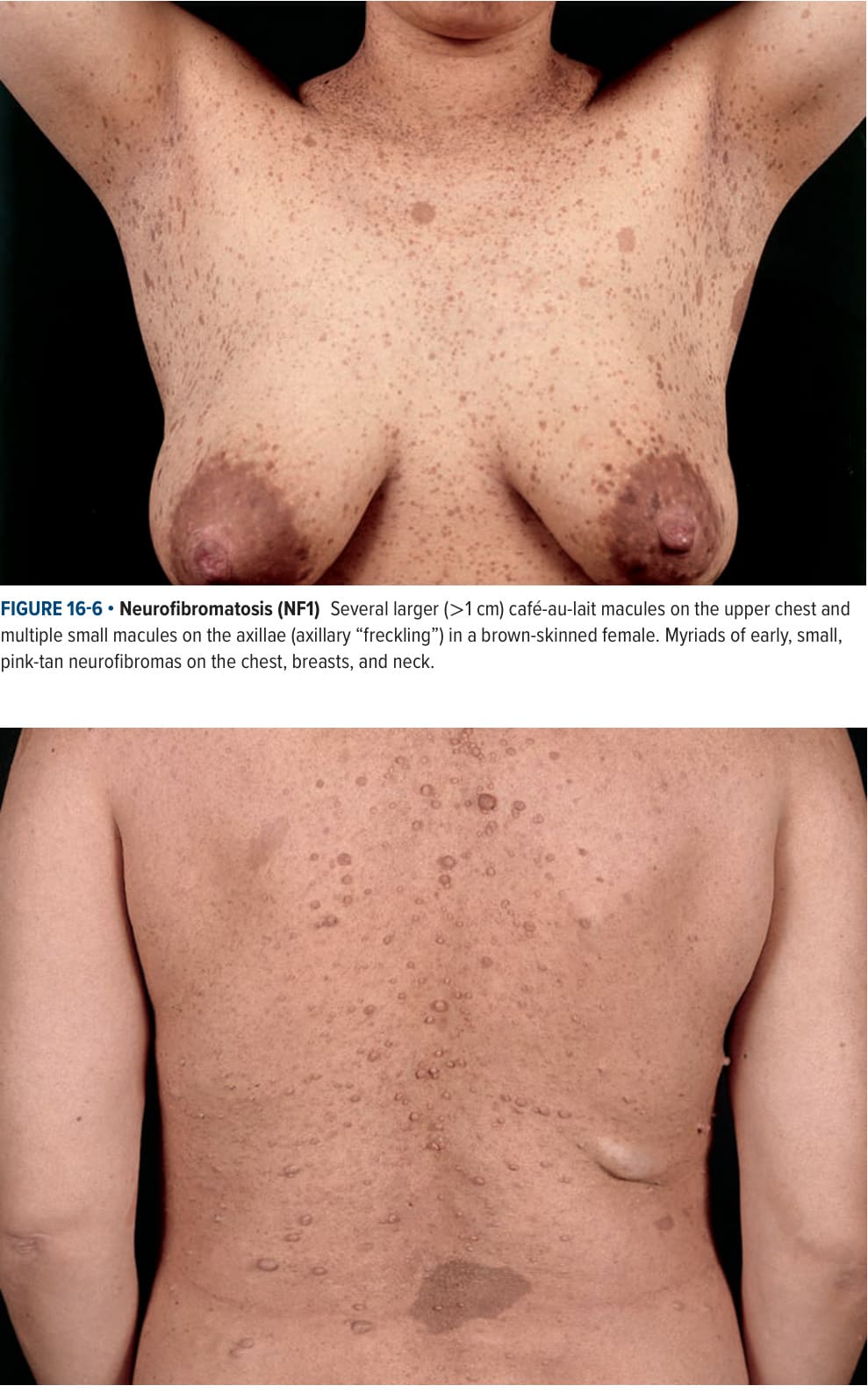
FIGURE 16-6 • Neurofibromatosis (NF1) Several larger (>1 cm) café-au-lait macules on the upper chest and multiple small macules on the axillae (axillary “freckling”) in a brown-skinned female. Myriads of early, small, pink-tan neurofibromas on the chest, breasts, and neck.
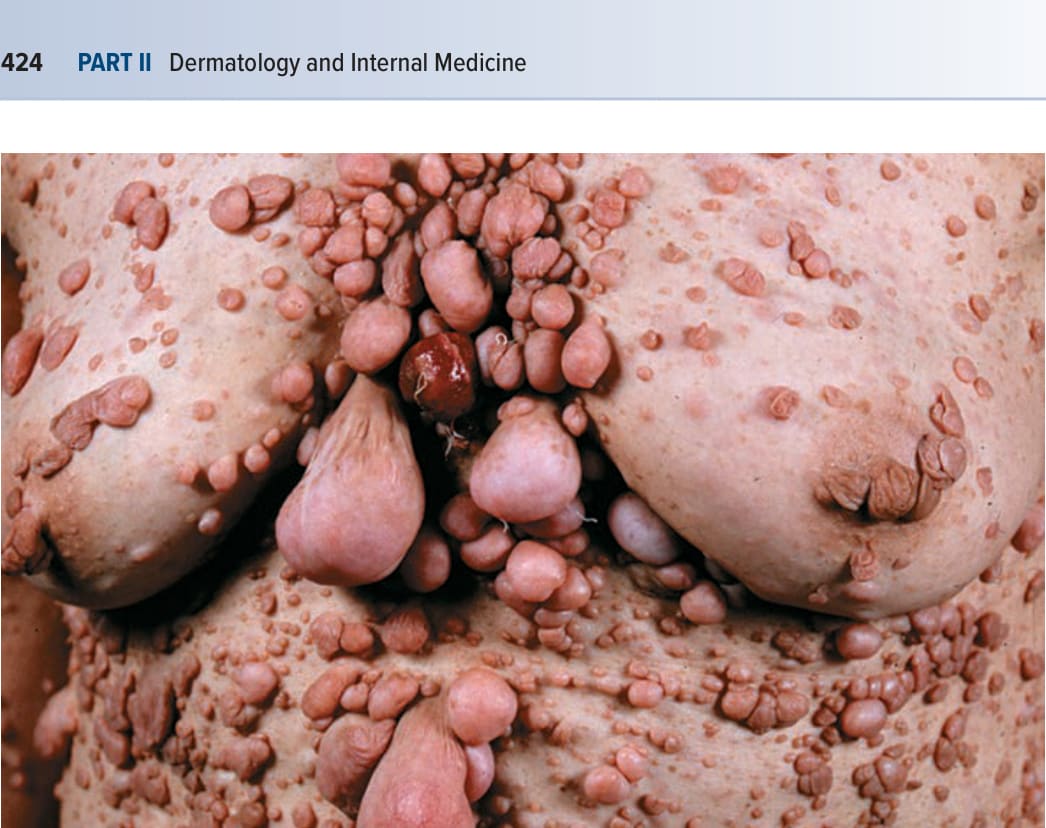
FIGURE 16-7 • Neurofibromatosis (NF1) Skin-colored and pink-tan, soft papules and nodules on the back are neurofibromas. The lesions first appeared during late childhood. One large café-au-lait macule on the back. The large, soft, ill-defined, subcutaneous nodule on the right lower back and on the right posterior axillary line are plexiform neuromas.

FIGURE 16-8 • Neurofibromatosis (NF1) An excessively large number of small and large, pedunculated neurofibromas on the chest of a 56-year-old woman who also had a severely distorted face caused by multiple neurofibromas and plexiform neuromas.

FIGURE 16-9 • Neurofibromatosis (NF1) Plexiform neuroma on the sole of the foot of a child. This ill-defined subcutaneous mass is soft and asymptomatic. The patient has café-au-lait macules and multiple neurofibromas.
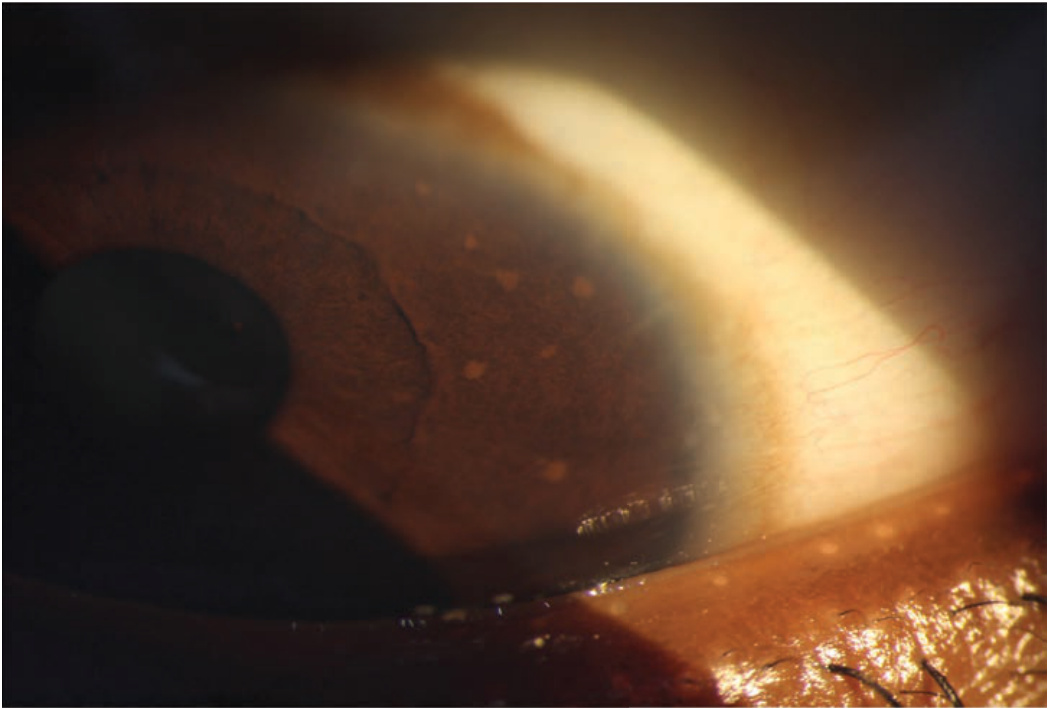
FIGURE 16-10 • Lisch nodules are visible only by slit-lamp examination and appear as “glossy” transient domeshaped yellow to brown papules of up to 2 mm.