THROMBOCYTOPENIC PURPURA
THROMBOCYTOPENIC PURPURA ICD-10: D69.3
• Thrombocytopenic purpura (TP) is characterized by cutaneous hemorrhages occurring in association with a reduced platelet count.
• Occur at sites of minor trauma/pressure (platelet count <40,000/μL) or spontaneously (platelet count <10,000/μL).
• Due to decreased platelet production, splenic sequestration, or increased platelet destruction.
• Decreased platelet production. Direct injury to bone marrow, drugs (cytosine arabinoside, daunorubicin, cyclophosphamide, busulfan, methotrexate, 6-mercaptopurine, vinca alkaloids, thiazide diuretics, ethanol, estrogens), replacement of bone marrow, aplastic anemia, vitamin deficiencies, and Wiskott–Aldrich syndrome.
• Splenic sequestration. Splenomegaly and hypothermia.
• Increased platelet destruction. Immunologic: Autoimmune TP, drug hypersensitivity (sulfonamides, quinine, quinidine, carbamazepine, digitoxin, or methyldopa), after transfusion. Nonimmunologic: Infection, prosthetic heart valves, disseminated intravascular coagulation, and thrombotic TP (microangiopathic hemolytic anemia, thrombocytopenia, neurologic abnormalities, fever and renal disease).
• Skin Lesions. Petechiae: Small (pinpoint to pinhead), red, nonblanching macules that are not palpable and turn brown as they get older (Fig. 20-1); later acquiring a yellowish-green tinge. Ecchymoses: Black-and-blue spots; larger area of hemorrhage. Vibices: Linear hemorrhages (Fig. 20-1), due to trauma or pressure. Most common on legs and upper trunk, but may occur anywhere.
• Mucous Membranes. Petechiae: Most often on palate (Fig. 20-2) and gingival bleeding.
• General Examination. Possible CNS and internal hemorrhage, anemia.
• Laboratory Hematology. Thrombocytopenia.
• Serology. Rule out HIV disease; antibodies against ADAMTS 13 (a protease).
• Lesional Skin Biopsy (bleeding usually can be controlled by suturing biopsied site) to rule out vasculitis.
• Differential diagnosis. Senile purpura, purpura of scurvy, progressive pigmentary purpura (Schamberg disease), purpura following severe Valsalva maneuver (coughing, vomiting/retching), traumatic purpura, factitial or iatrogenic purpura, and vasculitis.
• Management. Identify underlying cause and correct, if possible. Oral glucocorticoids, high-dose IV immunoglobulins, or platelet transfusion for chronic (Immune Thrombocytopenic Purpura) ITP (splenectomy may be indicated).

FIGURE 20-1 • Thrombocytopenic purpura Multiple petechiae on the upper arm of an HIV-infected 25-yearold male were the presenting manifestation of his disease. The linear arrangement of petechiae at the site of minor trauma is called vibices.
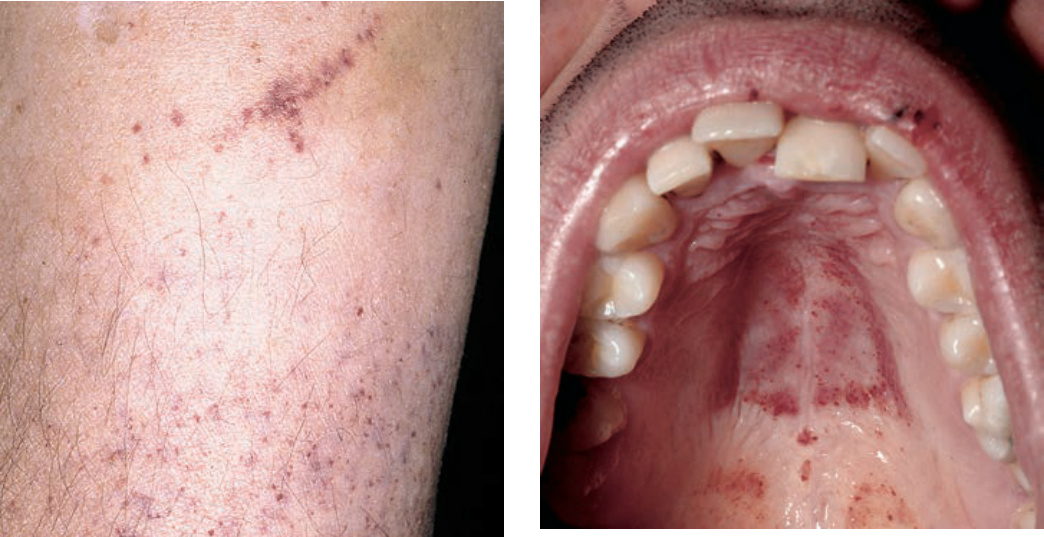
FIGURE 20-2 • Thrombocytopenic purpura Can first manifest on the oral mucosa or conjunctiva. Here, multiple petechial hemorrhages are seen on the palate.