CRYOGLOBULINEMIA
CRYOGLOBULINEMIA ICD-10: D89.1
• Cryoglobulinemia (CG) is the presence of serum immunoglobulin (precipitates at low temperature and redissolves at 37°C) complexed with other immunoglobulins or proteins.
• Associated clinical findings include purpura in cold-exposed sites, Raynaud phenomenon, cold urticaria, acral hemorrhagic necrosis, bleeding disorders, vasculitis, arthralgia, neurologic manifestations, hepatosplenomegaly, and glomerulonephritis.
• Precipitation of cryoglobulins (when present in large amounts) causes vessel occlusion, and is also associated with hyperviscosity.
• Platelet aggregation/consumption of clotting factors by cryoglobulins, causing coagulation disorder.
• Immune complex deposition followed by complement activation and vasculitis.
ETIOLOGY AND PATHOGENESIS
Type I Cryoglobulins: Monoclonal immunoglobulins (IgM, IgG, IgA, light chains). Associated with plasma cell dyscrasias such as multiple myeloma, Waldenström macroglobulinemia, lymphoproliferative disorders such as B cell lymphoma. Type II Cryoglobulins: Mixed cryoglobulins: Two immunoglobulin components, one of which is monoclonal (usually IgG, less often IgM) and the other polyclonal. Associated with multiple myeloma, Waldenström macroglobulinemia, chronic lymphocytic leukemia; rheumatoid arthritis, systemic lupus erythematosus, and Sjögren syndrome. Type III Cryoglobulins: Polyclonal immunoglobulins that form cryoprecipitate with polyclonal IgG or a nonimmunoglobulin serum component occasionally mixed with complement and lipoproteins. Represents immune complex disease. Associated with autoimmune diseases; connective tissue diseases; wide variety of infectious diseases, i.e., hepatitis B, hepatitis C, Epstein–Barr virus infection, cytomegalovirus infection, subacute bacterial endocarditis, leprosy, syphilis, and streptococcal infections.
CLINICAL MANIFESTATION
There is cold sensitivity in <50% of cases. Chills, fever, dyspnea, and diarrhea may occur following cold exposure. Purpura also may follow long periods of standing or sitting. Due to other organ system involvement, arthralgia, renal symptoms, neurologic symptoms, abdominal pain, and arterial thrombosis.
• Noninflammatory purpura (usually type I), occurring at cold-exposed sites, e.g., helix (Fig. 20-6) or the tip of the nose.
• Acrocyanosis and Raynaud phenomenon, with or without severe resultant gangrene of fingertips and toes or elsewhere on arms or legs (usually type I or II) (Fig. 20-7).
• Palpable purpura with bullae and necroses (usually types II and III) due to hypersensitivity vasculitis, occurring in crops on lower extremities with extension to thighs and abdomen; precipitated by standing up (Fig. 20-8), less commonly by cold.
B A
• Livedo reticularis mostly on extremities.
• Urticaria induced by cold, associated with purpura.
• Systemic involvement: Between 30% and 60% of individuals with essential mixed CG (type II) develop renal disease with hypertension, edema, or renal failure. Neurologic involvement manifests as peripheral sensorimotor polyneuropathy, presenting as paresthesias or foot drop. Arthritis. Hepatosplenomegaly.
• Diagnosis is confirmed by determination of cryoglobulins (blood drawn into warmed
syringe, RBC removed via warmed centrifuge; plasma refrigerated in a Wintrobe tube at 4°C for 24 to 72 hours, then centrifuged and cryocrit determined) and diagnosis of underlying disease.
• The course is characterized by cyclic eruptions induced by cold or fluctuations of the activity of the underlying disease.
• Treatment is that of the underlying disease. Idiopathic disease can be treated with plasmapheresis, oral corticosteroids, and mycophenolate mofetil.

FIGURE 20-6 • Cryoglobulinemia: Monoclonal (type I) This noninflamed, purpuric lesion on the helix appeared on the first cold day in the fall.
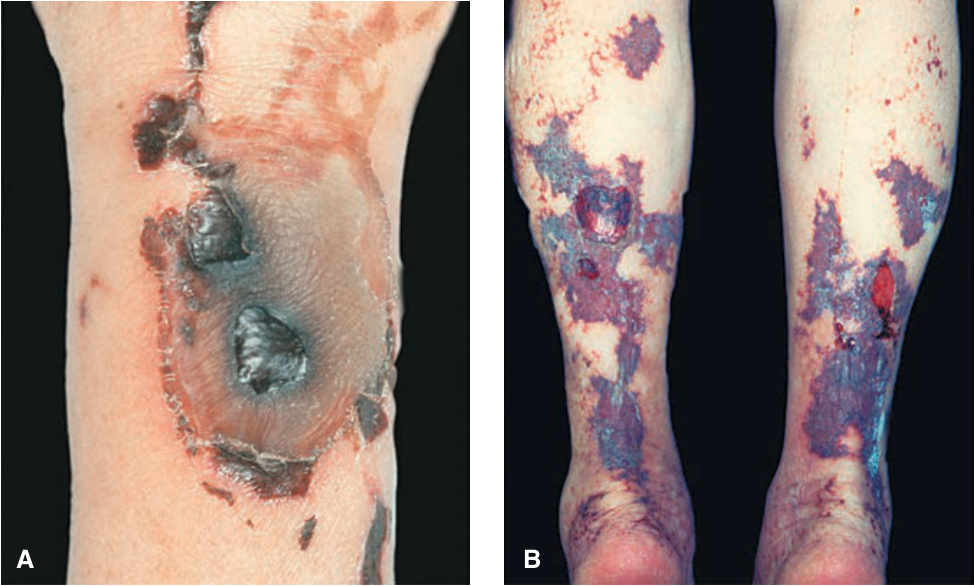
FIGURE 20-7 • Cryoglobulinemia: Mixed (type II) (A) Extensive necrosis and hemorrhage on the skin of the forearm. There was also digital gangrene on hands and feet. (B) Extensive hemorrhagic necrosis on both legs. There was also acral gangrene on four toes.
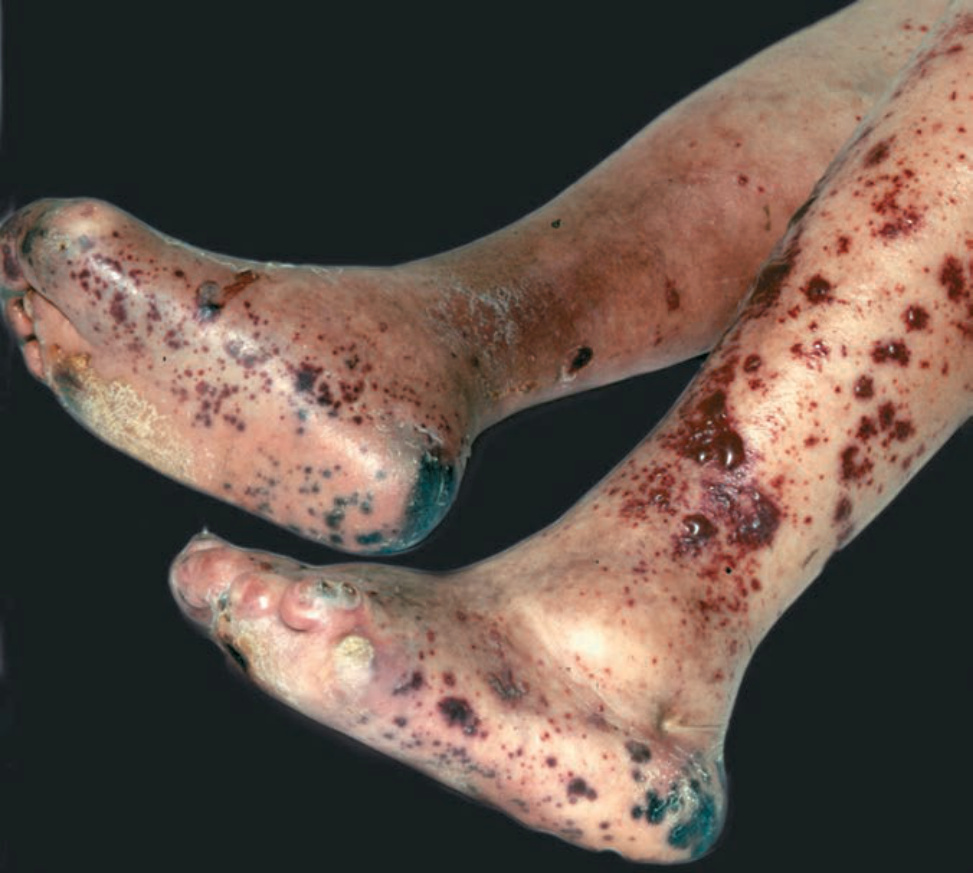
FIGURE 20-8 • Cryoglobulinemia: Polyclonal (type III) Palpable purpura with widespread hemorrhagic blisters and necrosis as in any other type of hypersensitivity vasculitis (compare with Fig. 14-51). Patient had diabetes and amputation of several toes.