LEUKEMIA CUTIS
LEUKEMIA CUTIS ICD-10: C92.3
• Leukemia cutis (LC) is a localized or disseminated skin infiltration by leukemic cells. It is usually a sign of dissemination of systemic disease or relapse of existing leukemia. The term aleukemic leukemia cutis describes a rare disorder in which extracutaneous evidence of recurrent leukemia cannot be ascertained. Prognosis tends to be poor.
• Incidence varies from <5% to 50%, depending on the type of leukemia, both acute and chronic, including the leukemic phase of non-Hodgkin lymphoma and hairy cell leukemia.
• Most commonly occurs with acute monocytic leukemia M5 and acute myelomonocytic leukemia M4.
• Most common lesions are small (2 to 5 mm) papules (Figs. 20-9 and 20-10), nodules (Figs. 20-11 and 20-12), or plaques. LC lesions are usually somewhat more pink, violaceous, or darker than normal skin, always palpable, indurated, and firm.
• Localized or disseminated; usually on the trunk (Fig. 20-9), extremities (Fig. 20-11), and the face (Fig. 20-10) but may occur at any site. May be hemorrhagic when associated with thrombocytopenia or may ulcerate (Fig. 20-12). Erythroderma may (rarely) occur. Leukemic gingival infiltration (hypertrophy) occurs with acute monocytic leukemia.
• Inflammatory disorders occurring in patients with leukemia are modified by the participation of leukemic cells in the infiltrate, resulting in unusual presentations of such disorders, e.g., psoriasis with hemorrhage or erosions/ulcerations.
• Cutaneous inflammatory diseases that may be associated with leukemia are Sweet syndrome, bullous pyoderma gangrenosum, urticaria, and necrotizing vasculitis.
• Systemic symptoms are those associated with hematologic malignancy.
• The diagnosis is made by suspicion and verified by skin biopsy, immunophenotyping, and B- or T-cell receptor rearrangement studies. Hematologic studies with complete analysis of bone marrow aspirate and peripheral blood smear.
• The prognosis for LC is directly related to the prognosis for the systemic disease.
• Therapy is usually directed at the leukemia itself. However, systemic chemotherapy sufficient for bone marrow remission may not treat the cutaneous lesions effectively. Thus, a combination of systemic chemotherapy and local electron beam therapy or (Psoralen plus Ultraviolet A) PUVA may be necessary for chemotherapy-resistant LC lesions. Intralesional chemotherapy has been used in management of localized, single, or a few lesions.

FIGURE 20-9 • Leukemia cutis Several tan-pink and violaceous papules and nodules on the trunk that arose very quickly. These lesions are “nonspecific” and do not present a diagnosis, but when such an eruption is seen, one should perform a peripheral blood count and a biopsy. (Used with permission of Dr. Kenneth Greer.)

FIGURE 20-10 • Leukemia cutis Multiple skin-colored and erythematous papules in a 38-year-old febrile woman that had erupted about 1 week before this picture was taken. The patient had acute myelogenous leukemia.
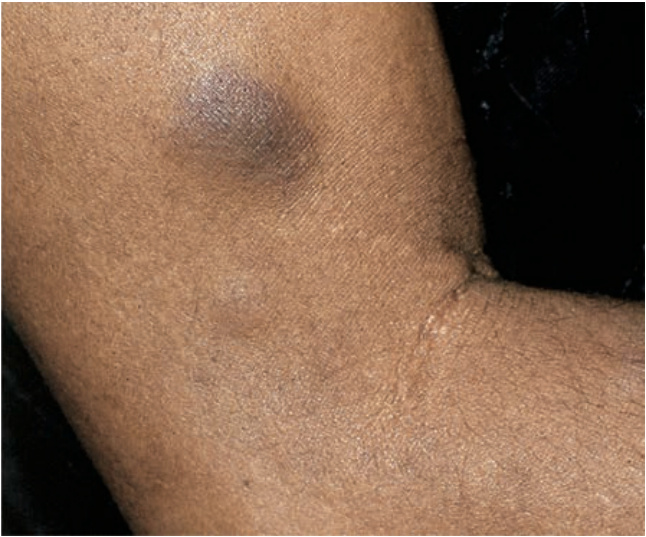
FIGURE 20-11 • Leukemia cutis A large, dark brown nodule on the upper arm of a male with acute myelogenous leukemia; six similar nodules were also present on the trunk.

FIGURE 20-12 • Leukemia cutis: Chloroma Large, ulcerated, green-hued tumors (chloromas) in the inguinal and perineal regions of a female with acute myelogenous leukemia; similar lesions were also present in the axillae and on the tongue.