MASTOCYTOSIS SYNDROMES
MASTOCYTOSIS SYNDROMES ICD-10: Q82.2
• Mastocytosis is an abnormal accumulation of mast cells in the skin and at various organs.
• An abbreviated WHO revised classification of mastocytosis is shown in Table 20-3.
• The skin is the most commonly involved organ system.
• Skin lesions are localized nodular or generalized maculopapular (Table 20-4).
• Because of the release of pharmacologically active substances, cutaneous symptoms are urticarial swelling or blistering with pruritus; systemic symptoms are blushing, vomiting, diarrhea, headache, and syncope.
• Most patients with mastocytosis have only skin involvement, and most of these have no systemic symptoms. However, up to half of patients with systemic mastocytosis may not have any skin findings.
Cutaneous mastocytosis (CM)
● Maculopapular cutaneous mastocytoma (urticarial pigmentosa)
● Disseminated cutaneous mastocytoma
● Mastocytoma of skin
Systemic Mastocytoma
● Indolent systemic mastocytosis (ISM)
● Smoldering systemic mastocytoma (SSM)
● Systemic mastocytosis with an associated clonal hematologic nonmast cell lineage disease (SM-AHNMD)
● Aggressive systemic mastocytosis (ASM)
● Mast cell leukemia (MCL)
Mast cell sarcoma (MCS)
Source: Adapted with permission from Valent P, Akin C, Metcalfe DD. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood. 2017; 129(11):1420–1427. Copyright © 2017 American Society of Hematology.
EPIDEMIOLOGY
AGE OF ONSET Between birth and 2 years of age (55%) (NCM, PPCM, UP), but mastocytosis can occur at any age; infancy-onset mastocytosis is rarely associated with systemic mastocytosis. SEX Slight male preponderance. PREVALENCE Unknown.
Localized Nodular CM (mastocytoma, NCM)
Generalized Maculopapular CM (MPCM) Papular plaque CM (PPCM) Urticaria pigmentosa (UP) Telangiectasia macularis eruptiva perstans (TMEP) Diffuse CM (DCM)
PATHOGENESIS
Human mast cell proliferation depends on the KIT ligand. Kit is the receptor for the stem cell factor. c-kit mutations have been identified in the blood and tissues of patients with mastocytosis. Mast cells contain several pharmacologically active substances that are associated with the clinical findings in mastocytosis: Histamine (urticaria or GI symptoms), prostaglandin D2 (flush, cardiovascular symptoms, bronchoconstriction, or GI symptoms), heparin (bleeding into tissue or osteoporosis), neutral protease/acid hydrolases (patchy hepatic fibrosis or bone lesions).
CLINICAL MANIFESTATION
Stroking lesion causes skin to itch and to wheal (Darier sign) (see generalized mastocytosis, below). Various drugs are capable of causing mast cell degranulation and release of pharmacologically active substances that
exacerbate skin lesions (whealing and itching) and cause flushing such as alcohol, dextran, polymyxin B, morphine, codeine, scopolamine, d-tubocurarine, and nonsteroidal anti-inflammatory drugs. Flushing episode can also be elicited by heat or cold and may be accompanied by headache, nausea, vomiting, diarrhea, dyspnea/wheezing, and syncope. Systemic involvement may lead to symptoms of malabsorption; portal hypertension. Bone pain. Neuropsychiatric symptoms (malaise and/or irritability). SKIN LESIONS (CM) LOCALIZED NCM Macular to papular to nodular lesions (mastocytoma) (Fig. 20-17), often solitary; may be multiple, but few. Yellow to tan-pink, which become erythematous and raised (urticate) when stroked due to degranulation of mast cells (Darier sign); in some patients, lesions become bullous. GENERALIZED PPCM Tan, occasionally yellowish plaques, up to 2 to 5 cm, sharply defined
with irregular outlines. Darier sign positive (Fig. 20-18). No scaling, occasionally with bulla formation after rubbing. Occurs mostly in infants and children.
MPCM/UP Tan macules to slightly raised tan to brown papules (Fig. 20-19). Disseminated, few or >100 with widespread symmetric distribution. Darier sign (whealing) after rubbing; in infants, may become bullous. Occurs in infancy and/or de novo in adults. Bright red diffuse flushing occurring spontaneously, after rubbing of skin, or after ingestion of alcohol or mast cell-degranulating agents.
TMEP Freckle-like, brownish to reddish macules (Fig. 20-20) with fine telangiectasia in long-standing lesions. Hundreds of lesions, on the trunk > extremities; lesions may be confluent. Urticate with gentle stroking. Dermatographism. Occur only in adults and very rare.
DCM Yellowish, thickened appearance of large areas of skin; “doughy.” Smooth with scattered elevation, resembling leather; “pseudoxanthomatous mastocytosis,” skin folds exaggerated,
especially in axilla/groin. Large bullae may occur after trauma or spontaneously. DCM may present as erythroderma (Fig. 20-21). Very rare, occurs at all ages.
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY Accumulation of normal- looking mast cells in dermis. Mast cell infiltrates may be sparse (spindle-shaped) or densely aggregated (cuboidal shape) and have a perivascular or nodular distribution. Various stains and immunoperoxidase methods can be used in difficult cases (metachromatic toluidine blue and Giemsa), such as tryptase and c-KIT. CBC Systemic mastocytosis: Anemia, leukocytosis, eosinophilia. BLOOD Tryptase levels ↑, coagulation parameters. URINE Patients with extensive cutaneous involvement may have increased 24-hour urinary histamine excretion. BONE SCAN AND IMAGING Define bone involvement (lytic bone lesions, osteoporosis, or osteosclerosis) and endoscopy for small-bowel involvement. BONE MARROW Smear and/or biopsy for morphology and mast cell markers.
DIAGNOSIS
Clinical suspicion, positive Darier sign, confirmed by skin biopsy.
DIFFERENTIAL DIAGNOSIS
NCM Juvenile xanthogranuloma, Spitz nevus. FLUSHING Carcinoid syndrome. MPCM/UP, PPCM, TMEP LCH, secondary syphilis, papular sarcoid, generalized eruptive histiocytoma, and non-LCH of childhood. DCM Cutaneous T-cell lymphoma, pseudoxanthoma elasticum, and forms of erythroderma.
COURSE AND PROGNOSIS
Most cases of solitary mastocytosis and generalized UP and PPCM in children resolve spontaneously. They rarely have systemic involvement. Adults with onset of MPCM/ UP or TMEP with extensive cutaneous involvement have a higher risk for development of systemic mastocytosis (see Table 20-3). In young children, acute and extensive degranulation may be life threatening (shock).
MANAGEMENT
Avoidance of drugs that may cause mast cell degranulation and histamine release (see the preceding). Antihistamines, both H1 and H2, either alone or with ketotifen. Disodium cromoglycate, 200 mg four times a day, may ameliorate pruritus, flushing, diarrhea, abdominal pain, and disorders of cognitive function but not skin lesions. Imatinib for patients with a KIT
mutation at the F522C position but ineffective with other KIT mutations. Midostaurin and avapritinib are FDA approved for treatment of aggressive SM and mast cell leukemia. PUVA treatment is effective for disseminated skin lesions, but recurrence is common. Vascular collapse is treated with epinephrine. NCM responds to potent glucocorticoid ointments under occlusion or to intralesional triamcinolone acetonide but may eventually recur.

FIGURE 20-17 • Mastocytosis: Solitary mastocytoma (NCM) A single, tan plaque with poorly demarcated borders on the posterior calf of an infant. When stroked vigorously, the lesion became erythematous, raised, and a blister developed. (Used with permission from Jennifer Tan, MD.)

FIGURE 20-18 • Mastocytosis: Generalized (PPCM) Multiple, flat-topped papules and small plaques of brownish to yellowish color on the buttocks of a child. Lesions are asymptomatic. Rubbing one of the lesions on the left buttock has resulted in urtication and an axon flare, a positive Darier sign, and itching.

FIGURE 20-19 • Mastocytosis: Urticaria pigmentosa (UP) Multiple, generalized tan to brown papules in a child. The patient had occasional syncopes, diarrhea, and wheezing; workup revealed systemic mastocytosis.
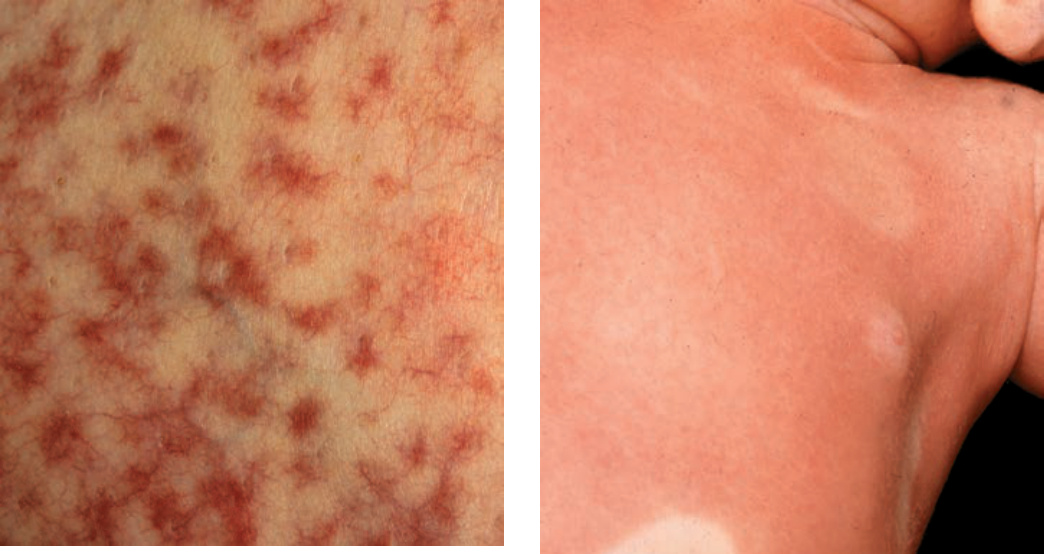
FIGURE 20-20 • Mastocytosis: Telangiectasia macularis eruptiva perstans (TMEP) Small, stellate erythematous macules and telangiectases on the back of a 45-year-old woman who had systemic (indolent) mastocytosis.

FIGURE 20-21 • Mastocytosis: Diffuse cutaneous mastocytosis (DCM) The skin of this infant is uniformly erythematous (erythroderma) secondary to infiltrating mast cells with several spared, white areas of normal skin. In this child, there were systemic symptoms associated with the flare of erythroderma: syncope, wheezing, and diarrhea.
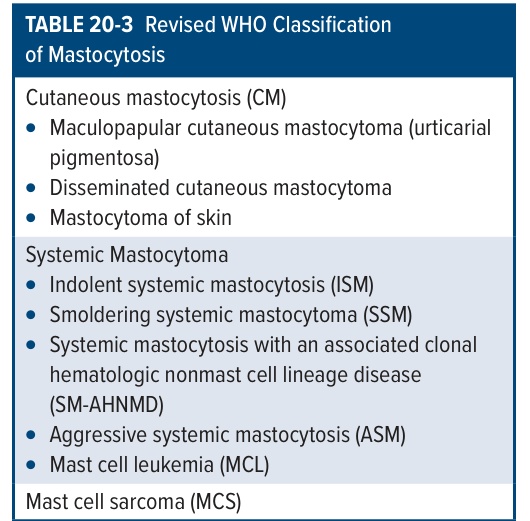
TABLE 20-3 Revised WHO Classification of Mastocytosis
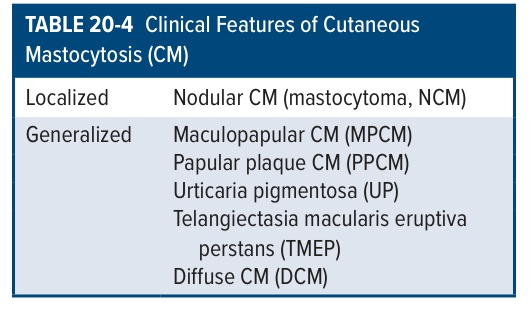
TABLE 20-4 Clinical Features of Cutaneous Mastocytosis (CM)