ADULT T-CELL LEUKEMIA/LYMPHOMA
ADULT T-CELL LEUKEMIA/LYMPHOMA ICD-10: C83/E88
• Adult T-cell leukemia/lymphoma (ATLL) is a neoplasm of CD4+/CD25+ T cells, caused by human T-cell lymphotropic virus I (HTLV-I).
• Manifested by skin infiltrates, hypercalcemia, visceral involvement, lytic bone lesions, and abnormal lymphocytes on peripheral smears.
• HTLV-I is a human retrovirus. Infection by the virus does not usually cause disease, which suggests that other environmental factors are involved. Immortalization of some infected CD4+ T cells, increased mitotic activity, genetic instability, and impairment of cellular immunity can all occur after infection with HTLV-I.
• ATLL occurs in southwestern Japan (Kyushu), Africa, the Caribbean Islands, and the southeastern United States. Transmission is by sexual intercourse, perinatally, or by exposure to blood or blood products (same as HIV).
• There are four main categories. In the relatively indolent smoldering and chronic forms, the median survival is ≥2 years. In the acute and lymphomatous forms, it ranges from only 4 to 6 months.
• Symptoms include fever, weight loss, abdominal pain, diarrhea, pleural effusion, ascites, cough, and sputum. Skin lesions occur in 50% of patients with ATLL. Single to multiple confluent erythematous, violaceous papules, ±purpura; firm violaceous to brownish nodules (Figs. 21-1 and 21-2); papulosquamous lesions, large plaques, ±ulceration; trunk > face > extremities; generalized erythroderma; poikiloderma; diffuse alopecia. Lymphadenopathy (75%) sparing mediastinal lymph nodes. Hepatomegaly (50%) and splenomegaly (25%).
• Patients are seropositive (ELISA, Western blot) to HTLV-I; in IV drug users, up to 30% have dual retroviral infection with both HTLV-I and HIV. WBC ranges from normal to 500,000/µL. Peripheral blood smears show polylobulated lymphocytic nuclei (“flower cells”). Dermatopathology reveals lymphomatous infiltrates composed of many large abnormal lymphocytes, ±giant cells, ±Pautrier microabscesses. There is hypercalcemia in 25% at time of diagnosis of ATLL and in >50% during clinical course; this is thought to be caused by osteoclastic bone resorption.
• Management consists of various regimens of cytotoxic chemotherapy; the rates of complete response are <30% and responses lack durability, but good results have been obtained with the combination of oral zidovudine and subcutaneous interferon-α in acute and lymphoma-type ATLL patients. Allogeneic hematopoietic stemcell transplantation has shown some promise.
CTCL
MF
MF variants
● Folliculotropic MF
● Pagetoid reticulosis
● Granulomatous slack skin
Sézary syndrome
Adult T-cell leukemia/lymphoma
Primary cutaneous CD30+ lymphoproliferative disorders
● Cutaneous anaplastic large cell lymphoma
● Lymphomatoid papulosis
Subcutaneous panniculitis-like T-cell lymphoma
Extranodal NK-T-cell lymphoma
Chronic active EBV infection
Primary cutaneous peripheral T-cell lymphoma
● Primary cutaneous γ/δ T-cell lymphoma
● CD8+ cutaneous aggressive epidermotropic T-cell lymphoma (provisional)
● Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (provisional)
● Primary cutaneous acral CD8+ T-cell lymphoma (provisional)
Primary cutaneous peripheral T-cell lymphoma, NOS
CBCL Primary cutaneous Marginal zone lymphoma Primary cutaneous follicular center lymphoma Primary cutaneous diffuse large B-cell lymphoma, leg type EBV + mucocutaneous ulcer (provisional) Intravascular large B-cell lymphoma
Source: Reproduced with permission from Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO- EORTC classification for primary cutaneous lymphomas. Blood. 2019; 133(16):1703–1714. Copyright © 2019 American Society of Hematology.
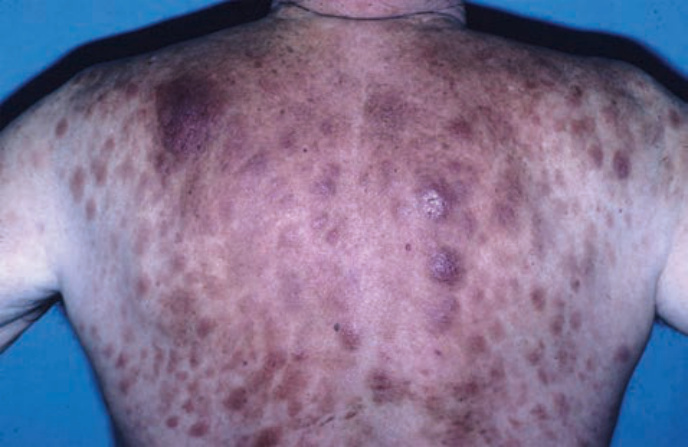
FIGURE 21-1 • Adult T-cell leukemia/lymphoma A generalized eruption of confluent violaceous papules with a predilection for the trunk. (Used with permission of Dr. Kenneth Greer.)

FIGURE 21-2 • Adult T-cell leukemia/lymphoma Firm, violaceous to brownish nodules as shown here are another cutaneous manifestation of ATLL. These nodules may ulcerate.
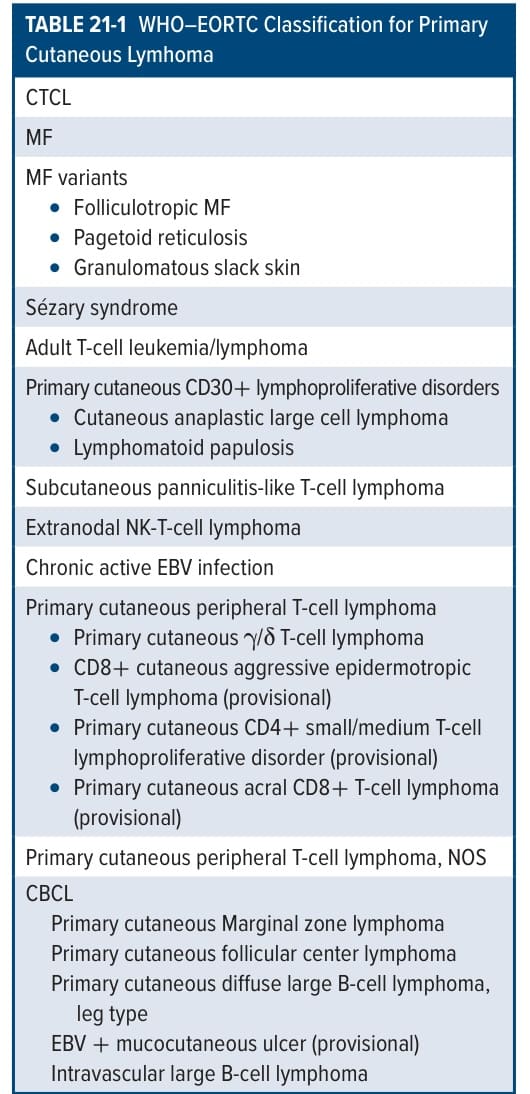
TABLE 21-1 WHO–EORTC Classification for Primary Cutaneous Lymhoma