MYCOSIS FUNGOIDES (MF)
MYCOSIS FUNGOIDES (MF) ICD-10: C84.0/C84.1
• MF is the most common cutaneous lymphoma.
• Arising in mid-to-late adulthood with male predominance of 2:1.
• A clonal proliferation of skin-homing CTLA+ CD4+ T cells with an admixture of CD8+ T cells (antitumor response).
• Categorized as patch, plaque, or tumor stage.
• Related features are pruritus, alopecia, palmoplantar hyperkeratosis, and bacterial infections.
• Histologically, epidermotropism of T cells with hyperconvoluted nuclei. In the tumor stage, dermal nodular infiltrates.
• Prognosis related to stage.
• Treatment: Symptom-oriented and stage-adapted.
EPIDEMIOLOGY AND ETIOLOGY
AGE OF ONSET Median age at diagnosis 55 to 60 years. SEX Male to female ratio 2:1. INCIDENCE Uncommon but not rare. ETIOLOGY Unknown. Cutaneous T-cell lymphoma (CTCL) is a malignancy of skin-homing CTLA+ CD4+ T cells.
CLINICAL MANIFESTATIONS
For months to years, often preceded by various diagnoses such as psoriasis, nummular dermatitis, and “large plaque” parapsoriasis. Symptoms: Pruritus, often intractable, but may be none. SKIN FINDINGS Skin lesions are classified into patches, plaques, and tumors. Patients may have simultaneously more than one type of lesion.
Patches Randomly distributed, scaling or nonscaling patches in different shades of red (Fig. 21-3). Well- or ill-defined; at first
superficial, much like eczema or psoriasis (Figs. 21-3 and 21-4) or mimicking dermatophytosis (“mycosis”), and later becoming thicker.
Plaques Round, oval, but often also arciform, annular, and of bizarre configuration (Figs. 21-3 and 21-4). Lesions are randomly distributed but in early stages often spare exposed areas.
Tumors Later lesions consist of nodules (Figs. 21-5 and 21-6) and tumors, with or without ulceration (Fig. 21-7). Extensive infiltration can cause leonine facies (Fig. 21-8). Confluence may lead to erythroderma (see Fig. 8-3). There is palmoplantar keratoderma and there may be hair loss. Poikiloderma may be present from the onset or develop later (Fig. 21-9). GENERAL EXAMINATION Lymphadenopathy, usually after thick plaques and nodules have appeared.
A B
A B
A B
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY Bandlike and patchy infiltrate in upper dermis of atypical lymphocytes (mycosis cells) extending to epidermis and skin appendages. The classic finding is the epidermotropism of this T-cell infiltrate, which will form microabscesses in the epidermis (Pautrier microabscesses). Fibroplasia of the upper dermis is often seen. Some cases fail to show significant lymphocytic atypia. In the plaque and tumor stage, the infiltrate extends deep into the dermis and beyond. Mycosis cells are T cells with hyperchromatic, irregularly shaped (cerebriform) nuclei. Mitoses vary from rare to frequent. Mycosis cells are activated monoclonal CTLA+ CD4+ T cells. HEMATOLOGY Eosinophilia, 6% to 12%, can increase to 50%. Buffy coat: Abnormal circulating T cells (mycosis cell type) and increased WBC (20,000/µL). Bone marrow examination is not helpful in early stages. Peripheral blood cytometry can also be helpful in detecting abnormal ratio of CD4+ cells. T-cell receptor studies can be used to detect clonal expansion. IMAGING In stage I and stage II disease, diagnostic imaging (CT, gallium scintigraphy,
liver–spleen scan, and lymphangiography) does not provide more information than biopsies of lymph nodes.
PET/CT Scan With more advanced disease; to search for retroperitoneal nodes in patients with extensive skin involvement, lymphadenopathy.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
In the early stages, the diagnosis of mycosis fungoides (MF) can be difficult. Clinical lesions may be typical, but histologic confirmation may not be possible for years despite repeated biopsies. Immunophenotyping of infiltrating T cells by use of monoclonal antibodies and T-cell receptor rearrangement studies. Lymphadenopathy and the detection of abnormal circulating T cells in the blood appear to correlate well with internal organ involvement. DIFFERENTIAL DIAGNOSIS Mainly scaling plaques. High index of suspicion is needed in patients with atypical or refractory “psoriasis,” “eczema,” and poikiloderma. MF often mimics psoriasis in being a scaly plaque and disappearing with exposure to sunlight.
Skin Body surface area assessment Routine histology Immunophenotyping Polymerase chain reaction for T-cell receptor rearrangement
Blood Complete blood count with smear examination Immunophenotyping
Lymph node Palpate all nodes Measure enlarged nodes by CT/PET scan Biopsy enlarged nodes
PATIENT EVALUATION IN MF AND STAGING The focus is on an evaluation of tumor burden, the degree of atypia of malignant cells, and the state of immunocompetence of the patient. Table 21-2 shows a flow sheet of patient evaluation, and Table 21-3 shows the TNM classification and staging of MF.
COURSE AND PROGNOSIS
Unpredictable; MF (pre-MF) may be present for years. Course varies with tumor stage and the source of the patients studied. Prognosis is much worse when (1) tumors are present (2) there is lymphadenopathy, (3) >10% of the skin surface is involved with pretumor-stage MF, and (4) there is a generalized erythroderma. Patients <50 years have twice the survival rate of patients >60 years.
MANAGEMENT
Therapy is symptom-oriented and extent of disease- and stage-adapted. In the pre-MF stage, in which the histologic diagnosis is only compatible, but not confirmed, PUVA photochemotherapy or narrowband UVB treatment is most effective. For histologically proven plaque-stage disease with no lymphadenopathy and no abnormal circulating T cells, PUVA photochemotherapy is also the method of choice, either alone or combined with oral isotretinoin or bexarotene or subcutaneous interferon-α. Also used at this stage are topical chemotherapy with nitrogen mustard in an ointment base (10 mg/dL),
Classification Definition
Stage
T1 Patches, plaques, or both involving <10% body-surface area T2 Patches, plaques, or both involving 10% or greater of body-surface area T3 One or more cutaneous tumors T4 Erythroderma N0 Lymph nodes clinically uninvolved N1 Lymph nodes clinically palpable but histologically uninvolved N2 Lymph nodes clinically nonpalpable but histologically involved N3 Lymph nodes clinically enlarged and histologically involved Nx Abnormal lymph nodes, no histology available M0 No visceral disease M1 Visceral disease B0 Less than 5% circulating atypical cells (Sézary cells) B1 More than 5% circulating atypical cells (Sézary cells) B2 High tumor burden (>1000/µL Sézary cells)
Clinical stage groups
IA T1N0M0 IB T2N0M0 IIA T1 or T2N1M0 IIB T3N0M0 or –T3N1M0 IIIA T4N0M0 IIIB T4N1M0 IVA T1 to 4N2 to 3 M0 IVB T1 to 4N0 to 3 M1
Source: Data from Olsen E et al: Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110:1713.
topical carmustine (BCNU) (for limited body surface area involvement), and total-body electron-beam therapy, singly or in combination, and methotrexate. Isolated tumors are treated with local x-ray or electron-beam therapy. For extensive plaque stage with multiple tumors or in patients with lymphadenopathy or abnormal circulating T cells, electron-beam plus chemotherapy is often used; randomized,
controlled studies of various combinations are in progress. Treatment escalation has included Histone deacetylase (HDAC) inhibitors such as vorinostat or romidepsin, brentuximab, mogamulizumab and standard chemotherapy with gemcitabine, doxorubicin, and chemotherapy
combination of Cyclophosphamide, Doxorubicin, Vincristine, Prednisone (CHOP). Stem-cell transplantation has been used with mixed results. Extracorporeal photophoresis and alemtuzumab are used in patients with Sézary syndrome, the leukemic form of the disease.

FIGURE 21-3 • Mycosis fungoides Lesions consist of randomly distributed, well- and/or ill-defined patches and later plaques. They may be scaly and appear in various shades of red. They mimic eczema, psoriasis, or dermatophytosis. (Used with permission of Dr. Kenneth Greer.)
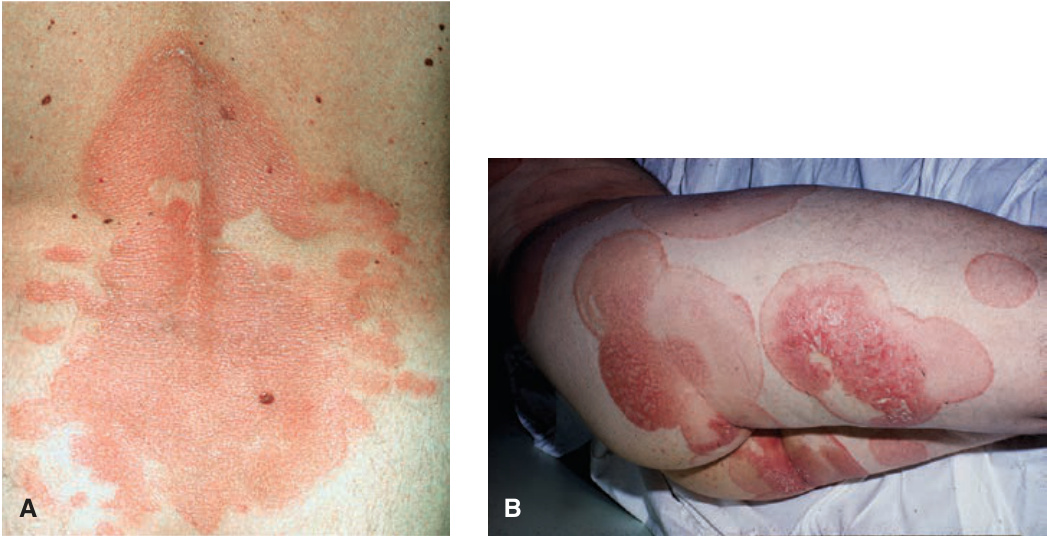
FIGURE 21-4 • (A) Mycosis fungoides: patches/plaque stage More advanced stages show confluence of patches and plaques with irregular configuration. This patient had been treated unsuccessfully for psoriasis for 2 years. Morphologically, he could also have extensive, confluent dermatophytosis (see Section 26), but a negative KOH preparation ruled out this diagnosis. Only after a biopsy had been done was the correct diagnosis of MF made. (B) 52-year-old man with patch and plaque stage MF that was previously diagnosed as tinea corporis.

FIGURE 21-5 • Mycosis fungoides Plaque and early nodular stage with reddish-brownish, scaly disease. (Used with permission of Dr. Kenneth Greer.)

FIGURE 21-6 • (A) Mycosis fungoides: tumor stage Scaly and crusted eczema-like plaques seen on the arm and chest have turned nodular on the shoulder. This patient had similar lesions elsewhere and was staged IIB (T3 N1 M0). (B) 62-year-old man with tumor stage MF.

FIGURE 21-7 • Mycosis fungoides: tumors Two large ulcerated tumors on the lower leg of a 58-year-old man. These lesions look like mushrooms.

FIGURE 21-8 • Mycosis fungoides: leonine facies In this patient, the disease had started with generalized eczema-like plaques on the trunk. Massive nodular infiltration of the face occurred leading to a leonine facies. (Used with permission of Dr. Kenneth Greer.)

FIGURE 21-9 • Mycosis fungoides: poikilodermatous lesions (A) Small reticulated, confluent papules mixed with superficial atrophy give the impression of poikiloderma. This patient had patches elsewhere on the body similar to those shown in Figure 21.4. (B) Poikiloderma in MF can also result from treatment. This patient had been treated with electron beam.
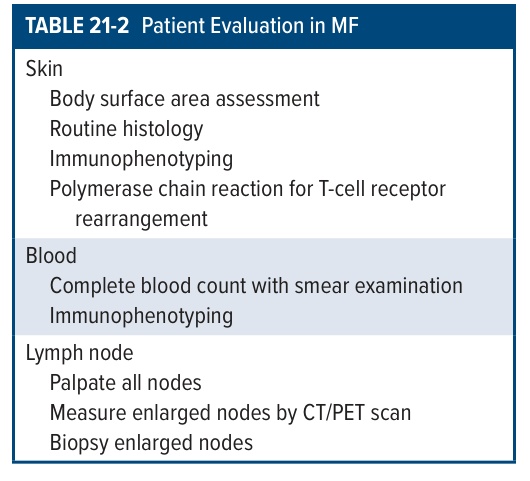
TABLE 21-2 Patient Evaluation in MF
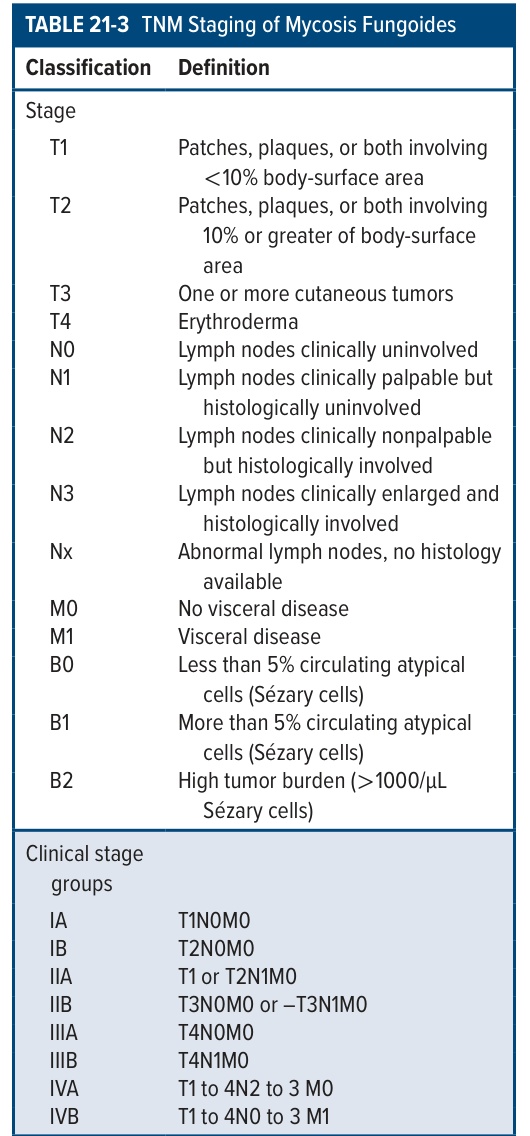
TABLE 21-3 TNM Staging of Mycosis Fungoides