LYMPHOMATOID PAPULOSIS
LYMPHOMATOID PAPULOSIS ICD-10: L41.2
• Lymphomatoid papulosis is an asymptomatic, chronic, self-healing, polymorphous eruption of unknown etiology.
• The WHO–EORTC classification in 2018 considers it a self-limited T-cell lymphoma with a low but real risk of progression to more malignant forms of lymphoma. It belongs in the spectrum of primary cutaneous CD30+ lymphoproliferative disorders.
• Incidence is 1.2 to 1.9 cases per million, occurring sporadically in both sexes from childhood to old age; average age 40 years.
• Characterized by recurrent crops of lesions that regress spontaneously, with histologic features of lymphocytic atypia.
• Close clinical resemblance to pityriasis lichenoides et varioliformis acuta (see Fig. 3.23 in Section 3). Erythematous to red-brown papules (Fig. 21-13) and nodules, 2 to 5 mm in diameter, which are initially smooth and hemorrhagic, later hyperkeratotic, with central, black necrosis, crusting (Fig. 21-13), and ulceration. Few to hundreds of lesions, asymptomatic or pruritic, arranged at random and often grouped, recurrent, primarily on trunk and extremities; rarely, oral and genital mucosa. Individual lesions evolve over a 2- to 8-week period and resolve spontaneously. Atrophic hyper- or hypopigmented scarring following ulcerated lesions.
• Other organ systems are uninvolved.
• Dermatopathology: Superficial or deep, perivascular or interstitial mixed-cell infiltrate, or wedge-shaped. Atypical cells may comprise 50% of infiltrate. Type A: Large CD30+, atypical histioid lymphocytes with abundant cytoplasm and convoluted nucleus. Type B: Smaller CD30–, atypical lymphocytes with cerebriform nuclei. Type C: Large CD30+ cells form sheets resembling cutaneous anaplastic large cell lymphoma (CALCL, see p. 496). D and E subtypes (CD4-/CD8+) have also been described.
• Differential diagnosis: Based on typical histology and immunohistochemistry; lack of systemic involvement by history and physical examination.
• Course: May remit in 3 weeks or continue for decades. In 10% to 20% of patients, lymphomatoid papulosis is preceded by, associated with, or followed by another type of lymphoma: MF, Hodgkin disease, or CD30+CALCL. Lymphomatoid papulosis (LyP) may rarely persist despite systemic chemotherapy for concurrent lymphoma.
• No treatments have proved consistently effective. Topical agents include corticosteroids and carmustine (BCNU). Electron-beam irradiation, PUVA. Retinoids, methotrexate, chlorambucil, cyclophosphamide, cyclosporine; brentuximab, and interferon-α2b, none with lasting effect.
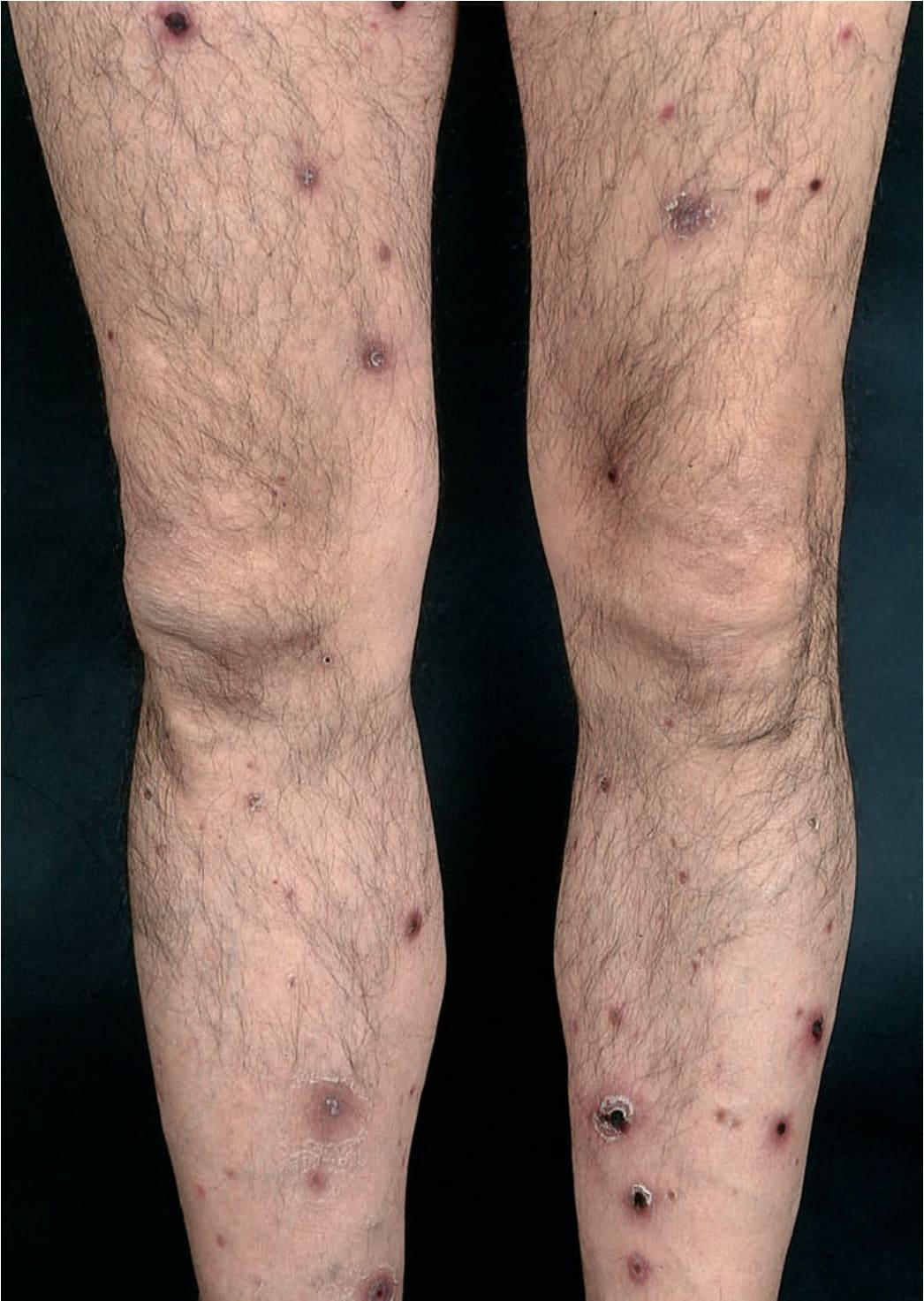
FIGURE 21-13 • Lymphomatoid papulosis Crops of reddish-brown papules appear in waves involving the entire body. Lesions are asymptomatic, become hyperkeratotic, crusted, and necrotic in the center. Since lesions arise asynchronously, all stages in this evolution are present simultaneously.