KAPOSI SARCOMA (KS)
KAPOSI SARCOMA (KS) ICD-10: C46
• KS is a multifocal systemic tumor of endothelial cell origin.
• Invariably linked with human herpes virus type 8 (HHV-8) infection.
• Four clinical variants: Classic KS, endemic African KS, immunosuppressive therapy-related KS (iatrogenic), and HIV/AIDS-related KS (epidemic).
• Stage- and variant-dependent localized and/or generalized disease: patches, plaques, and nodules.
• Systemic involvement: Mainly GI tract and lung.
• Responds to radiation and chemotherapy.
ETIOPATHOGENESIS
DNA of HHV-8 has been identified in tissue samples of all variants of Kaposi sarcoma (KS).
CLASSIFICATION AND CLINICAL VARIANTS
CLASSIC OR EUROPEAN KS Occurs in elderly males of eastern European heritage (Mediterranean and Ashkenazi Jewish). Not so uncommon in eastern and southern Europe; rare in the United States. Males > females. Predominantly arises on the legs but also occurs in lymph nodes and abdominal viscera; slowly progressive. AFRICAN-ENDEMIC KS Between 9% and 12.8% of all malignancies in sub-Saharan Africa. Two distinct age groups: young adults, mean age 35; and young children, mean age 3 years. Males > females. No evidence of underlying immunodeficiency. Four clinical patterns (see below). IATROGENIC IMMUNOSUPPRESSION-ASSOCIATED KS RARE Most commonly in solid-organ transplant recipients as well as individuals treated chronically with immunosuppressive drugs. Arises on average 16.5 months after transplantation. Resolves on cessation of immunosuppression. HIV/AIDS-ASSOCIATED KS In HIV-infected individuals, the risk for KS is 20,000 times than that of the general population, 300 times than that of other immunosuppressed individuals. Despite a decline in recent years, KS is still the most common tumor in male patients with AIDS. Less commonly, women may have HIV/ AIDS-associated KS. Associated with HIV infection, rapid progression, and extensive systemic involvement. At the time of initial presentation, one in six HIV-infected individuals
with KS have CD4+ T-cell counts of ≤500/µL. However, as of late, tumors have been reported significantly after reconstitution. Rare variants have recently permeated the literature, in non-HIV–infected, non-Mediterranean, noniatrogenically immunosuppressed patients. Generally, young men appear over represented in these rare cohorts.
PATHOGENESIS
KS cells are likely derived from the endothelium of the blood/lymphatic microvasculature. KS lesions produce factors that promote their own growth as well as the growth of other cells, but it is not clear how HHV-8 induces/ promotes proliferation of endothelial cells.
CLINICAL MANIFESTATION
Mucocutaneous lesions are usually asymptomatic but are associated with significant cosmetic stigma. At times, lesions may ulcerate and bleed easily. Large lesions on the palms or soles may impede function. Lesions on the lower extremities that are tumorous, ulcerated, or associated with significant edema often give rise to moderate-to-severe pain. Urethral or anal canal lesions can be associated with obstruction. GI involvement rarely causes symptoms but can lead to obstruction and bleeding in late stages. Pulmonary KS can cause bronchospasm, intractable coughing, shortness of breath, and progressive respiratory failure. SKIN LESIONS KS most often begins as an ecchymotic-like macule/papule (Fig. 21-16). Macules evolve into patches, papules, plaques (Figs. 21-16 to 21-18), nodules, and tumors that are violaceous, red, pink, or tan and
A B
become purple-brownish (Figs. 21-16 and 21-19) with a greenish hemosiderin halo as they age. Often oval initially, and on the trunk often arranged parallel to skin tension lines (Fig. 21-20). Lesions may initially occur at sites of trauma, usually in the acral regions (Fig. 21-18). In time, individual lesions may enlarge and become confluent, forming tumor masses. Secondary changes to larger nodules and tumors include erosion, ulceration, crusting, and hyperkeratosis. Lymphedema usually occurs on the lower extremities (Figs. 21-17 and 21-19) and results from confluent masses of lesions caused by deeper involvement of lymphatics and lymph nodes. Distal edema may initially be unilateral but later becomes symmetric and involves not only the lower legs but also the genitalia and/or face.
Distribution Widespread or localized. In classic KS, lesions almost always occur on the feet and legs or the hands, and slowly spread centripetally (Figs. 21-16 and 21-19). The tip of the nose (Fig. 21-17), periorbital areas, ears, and scalp as well as penis and legs may also be involved, but involvement of the trunk is rare. In HIV/AIDS-associated KS, there is early involvement of the face and widespread distribution on the trunk (Fig. 21-20).
MUCOUS MEMBRANES Oral lesions are the first manifestation of KS in 22% of cases; HIV/ AIDS-associated KS is often a marker for CD4+ T-cell counts of <200/µL but exceptions exist. Very common (50% of individuals) on the hard palate, appearing first as a violaceous stain, which evolves into papules and nodules with a cobblestone appearance (see Section 33). Lesions also arise on soft palate, uvula, pharynx, gingiva, and tongue. Conjunctival lesions are uncommon.
Special Features of African-Endemic KS (non- HIV associated). Four clinical patterns are recognized:
• Nodular type: Runs a rather benign course with a mean duration of 5 to 8 years and resembles classic KS.
• Florid or vegetating type: Characterized by more aggressive biologic behavior; it is also nodular but may extend deeply into the subcutis, muscle, and bone.
• Infiltrative type: Shows an even more aggressive course with florid mucocutaneous and visceral involvement.
• Lymphadenopathic type: Predominantly affects children and young adults. Frequently confined to lymph nodes and viscera, but occasionally also involves the skin and mucous membrane. GENERAL EXAMINATION Viscera KS lesions of the viscera, though common, are often asymptomatic. This is particularly true for classic KS. An autopsy of HIV-infected individuals with mucocutaneous KS, reveal that 75% have visceral involvement (bowel, liver, spleen, or lungs).
Lymph Nodes Lymph nodes are involved in half of the cases of HIV/AIDS-associated KS and in all cases of African lymphadenopathic type KS.
Urogenital Tract Prostate, seminal vesicles, testes, bladder, penis, and scrotum.
Lung Pulmonary infiltrates, particularly in HIV-associated KS.
GI Tract GI hemorrhage, rectal obstruction, protein-losing enteropathy can occur.
Other Heart, brain, kidney, and adrenal glands.
LABORATORY EXAMINATIONS
SKIN BIOPSY Vascular channels lined by atypical endothelial cells among a network of reticulin fibers and extravasated erythrocytes with hemosiderin deposition. In the nodular stage: Spindle cells in sheets and fascicles with mild-to-moderate cytologic atypia, single cell necrosis, trapped RBCs within an extensive network of slit-like vascular spaces. Stains against HHV-8 can be used in cases where diagnostic uncertainty exists. IMAGING For internal organ involvement.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Confirmed on lesional skin biopsy. DIFFERENTIAL DIAGNOSIS Includes single pigmented lesions: Dermatofibroma, pyogenic granuloma, hemangioma, bacillary (epithelioid) angiomatosis, melanocytic nevus, ecchymosis, granuloma annulare, insect bite reactions, and stasis dermatitis.
COURSE AND PROGNOSIS
CLASSIC KS Average survival, 10 to 15 years; death usually from unrelated causes. Secondary malignancies arise in >35% of cases. AFRICAN-ENDEMIC KS Mean survival in young adults, 5 to 8 years; young children, 2 to 3 years. IATROGENIC IMMUNOSUPPRESSION-ASSOCIATED KS The course may be chronic or rapidly progressive; KS usually resolves after immunosuppressive drugs are discontinued.
HIV/AIDS-Associated KS (see also Section 27). HIV-infected individuals with high CD4+ T-cell counts can have stable or slowly progressive disease for many years. Rapid progression of KS can occur after decline of CD4+ T-cell counts to low values, prolonged systemic glucocorticoid therapy, or illness such as Pneumocystis jiroveci pneumonia. KS of the bowel and/or lungs is the cause of death in 10% to 20% of patients. Patients with only a few lesions, present for several months, without history of opportunistic infections, and CD4+ T-cell counts >200/µL tend to respond better to therapy and have a better overall prognosis. At time of initial diagnosis, 40% of KS patients have GI involvement; 80% at autopsy. Reduced survival rate is seen in patients with GI involvement. Pulmonary KS
has high short-term mortality rate, that is, median survival <6 months.
MANAGEMENT
The goal of therapy for KS is to control symptoms of the disease, not cure. A number of local and systemic therapeutic modalities are effective in controlling symptoms. Classic KS responds well to radiotherapy of involved sites. African-endemic KS, when symptomatic, responds best to systemic chemotherapy. Immunosuppressive drug-associated KS regresses or resolves when drug dosages are reduced or discontinued. HIV/AIDS-associated KS usually responds to a variety of local therapies; for extensive mucocutaneous involvement or visceral involvement, chemotherapy is indicated. Of course, all this is in addition to anti retroviral therapy, the most effective therapy.
Limited Intervention
RADIOTHERAPY Indicated for tumorous lesions, confluent lesions with a large surface area, large lesions on distal extremity, and large oropharyngeal lesions. Cryosurgery Indicated for deeply pigmented, protruding nodules. Laser Surgery Pulsed-dye laser effective for small superficial lesions. Photodynamic Therapy For small superficial lesions. ELECTROSURGERY Effective for ulcerated, bleeding nodular lesions. Excisional Surgery Effective for selected small lesions. Intralesional Cytotoxic Chemotherapy Vinblastine, Vincristine, and Bleomycin.
Aggressive Intervention
Single-Agent Chemotherapy With adriamycin, vinblastine, lipid formulations of daunorubicin, and doxorubicin. Paclitaxel (Taxol), thalidomide, and col-3. Combination Chemotherapy Vincristine + bleomycin + adriamycin or interferon-α+ zidovudine.
Type-Specific Therapy
• Classic KS: Any of the preceding.
• African KS: Any of the preceding.
• Immunosuppression-related KS: Reduction in immunosuppression, replacement of calcineurin inhibitors by rapamycin.
• HIV/AIDS-related KS: Any of the preceding, preferably liposomal anthracyclines intravenously plus HAART.

FIGURE 21-16 • Classic Kaposi sarcoma Ecchymotic purple-reddish confluent macules and papules on the dorsum of the hand. The lesion was originally mistaken for a bruise as were similar lesions on the feet and on the other hand. The patient was otherwise asymptomatic.

FIGURE 21-17 • HIV/AIDS-associated Kaposi sarcoma (A) Multiple violaceous papules and nodules, some coalescing and spontaneously ulcerative. Infiltration is noted surrounding the primary lesion. The leg has become edematous caused by lymphatic involvement. (B) In more advanced cases, complete obliteration of lymphatic vessels leads to an elephantiasis-like picture, often asymmetrical. Discrete violaceous papulonodules can still be seen. (Used with permission from Adam Lipworth, MD.)

FIGURE 21-18 • Classic Kaposi sarcoma of the feet Brownish to blue nodules and plaques, partial-ly hyperkeratotic on the soles and lateral aspects of the feet. This is a typical localization of early classic KS.
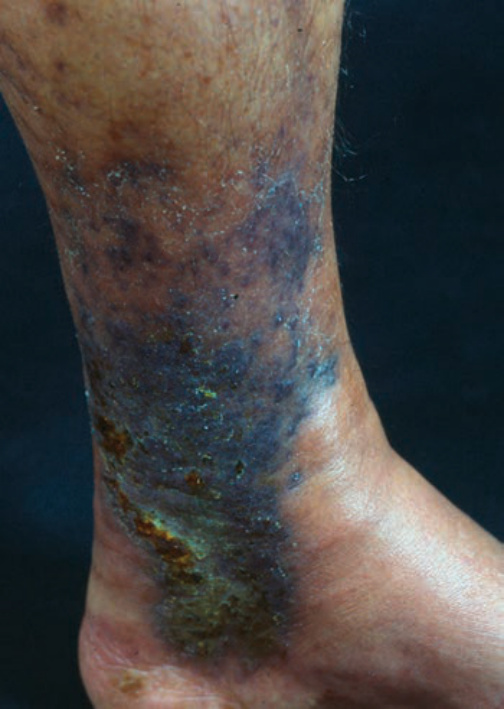
FIGURE 21-19 • Classic Kaposi sarcoma Black confluent papules on the lower leg that are reminiscent of hyperpigmented stasis dermatitis in chronic venous insufficiency. Involvement of lymphatics has led to pronounced edema of the calf. This indicates that the disease process is further advanced.

FIGURE 21-20 • HIV/AIDS-associated Kaposi sarcoma Multiple purplish plaques and nodules on the chest of a homosexual AIDS patient. The patient had CD4+ T-cell counts <200/µL. (Used with permission from Adam Lipworth, MD.)