PUSTULAR ERUPTIONS
PUSTULAR ERUPTIONS ICD-10: T88.7
• Acute generalized exanthematous pustulosis (AGEP) is an acute febrile eruption that is often associated with leukocytosis (Fig. 23-2). After drug administration, it may take 1 to 3 weeks before skin lesions appear. However, in previously sensitized patients, the skin symptoms may occur within 2 to 3 days.
• Onset is acute, most often following drug intake, but viral infections can also trigger the disease.
• AGEP typically presents with nonfollicular sterile pustules occurring on a diffuse, edematous erythema (Fig. 23-2).
• May be irregularly dispersed or grouped (Fig. 23-3A), usually starting in the folds (Fig. 23-3B) and/or the face.
• Fever and elevated blood neutrophils are common.
• Histopathology typically shows spongiform subcorneal and/or intraepidermal pustules; a marked edema of the papillary dermis; and eventually vasculitis, eosinophils, and/or focal necrosis of keratinocytes.
• Pustules resolve spontaneously in <15 days and generalized desquamation occurs approximately 2 weeks later.
• Differential diagnosis includes pustular psoriasis, the hypersensitivity syndrome reaction with pustulation, subcorneal pustular dermatosis (Sneddon–Wilkinson disease), and pustular vasculitis.
• Acneiform pustular eruptions (see Section 1) are associated with iodides, bromides, adrenocorticotropic hormone (ACTH), glucocorticoids, isoniazid, androgens, lithium, actinomycin D, and phenytoin. The EGFR tyrosine kinase inhibitors erlotinib, gefitinib, cetuximab, and panitumumab produce pustules that are acneiform but without comedones and erupt in the face (Fig. 23-4A) but can erupt also in atypical areas, such as on the arms and legs (Fig. 23-4B), and are most often monomorphous.
A B
A B
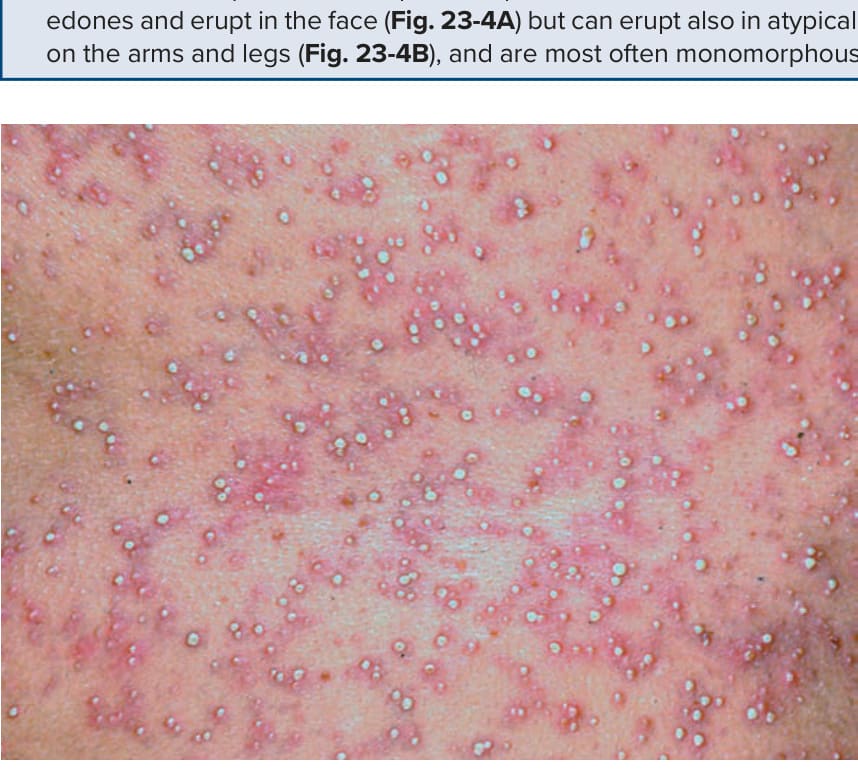
FIGURE 23-2 • Pustular drug eruption: acute generalized exanthematous pustulosis (AGEP) Multiple tiny nonfollicular pustules against the background of diffuse erythema that first appeared in the large folds and then covered the entire trunk and the face.
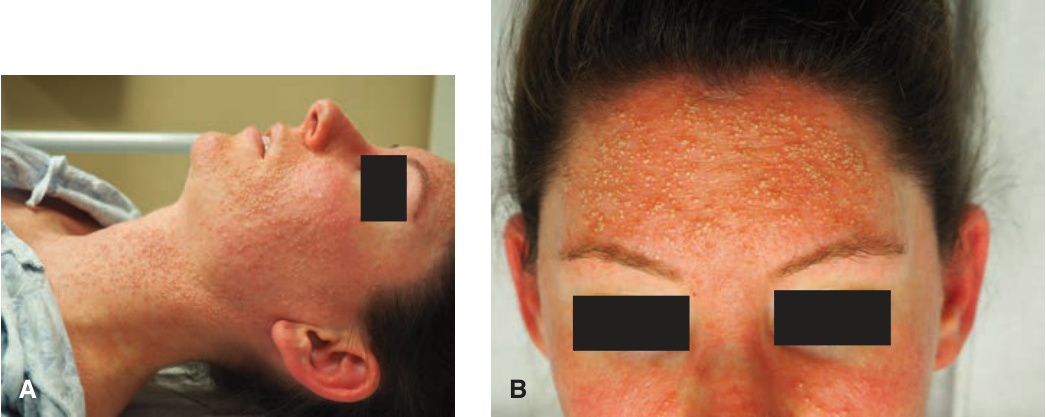
FIGURE 23-3 • Pustular drug eruption: AGEP (A) Multiple sterile pustules surrounded by fiery-red erythema who had fever and leukocytosis. In contrast to the disseminated pustules in Figure 23-2, here the pustules show a tendency for grouping and confluence. Differential diagnosis includes von Zumbusch pustular psoriasis (compare with Fig. 3-12). (B) Pustules are often noted in the axilla and skin folds.
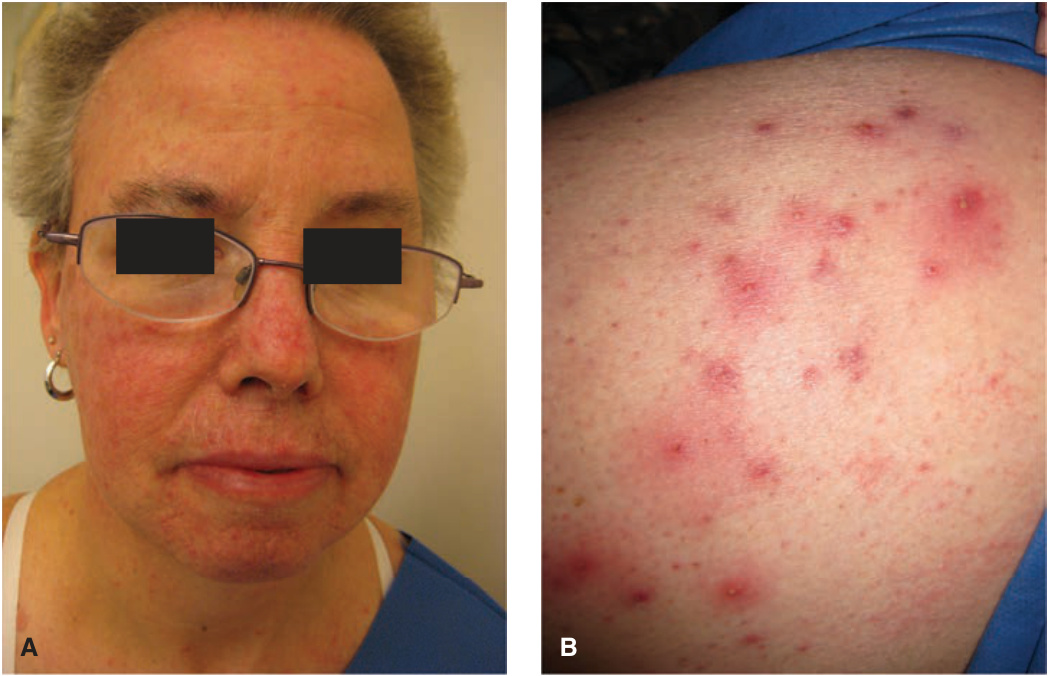
FIGURE 23-4 • Pustular drug eruption: erlotinib (A) This pustular eruption occurred in a patient who had received an anti-EGR monoclonal antibody for cancer of the lung. Differential diagnosis includes acne and rosacea. (B) More inflammatory lesions are noted in the upper thigh with intense surrounding erythema.