ACDR-RELATED TO CHEMOTHERAPY
ACDR-RELATED TO CHEMOTHERAPY ICD-10: T88.7
• Chemotherapy may induce local and systemic skin toxicity with a wide range of cutaneous manifestations from benign to life threatening.
• The ACDR can be related to overdose, pharmacologic side effects, cumulative toxicity, delayed toxicity, or drug–drug interactions.
• Clinical manifestations range from alopecia (see Section 31) and nail changes (see Section 32) to acral erythema, often with sensory abnormalities: Palmoplantar dysesthesia (capecitabine, cytarabine, doxorubicin, fluorouracil). Other notable features include paronychia (Fig. 23-18A), trichomegaly (Fig. 23-18B) and acneiform/pustular reactions of signal transduction inhibitors such as erlotinib (Fig. 23-19A). Mucositis is also very common and can often lead to erosive disease (Fig. 23-19B).
• Chemotherapeutic agents are also responsible for inflammation and ulceration at sites of extravasation of intravenous medications, such as doxorubicin or taxol, which can be followed by skin necrosis.
• Other reactions are radiation recall or enhancement (as with methotrexate), erosion or ulceration of psoriasis caused by an overdose of methotrexate, inflammation, and sloughing of actinic keratosis resulting from 5-fluorouracil or fludarabine, or erosions caused by cisplatin plus 5-fluorouracil.
• Table 23-7 lists newer chemotherapeutics including “biologicals” and their ACDR.
A B
A B
Class Agents ACDRa
Spindle inhibitor Taxanes: docetaxel, paclitaxel Hand-foot skin reactionb; combined with sensory abnormalities: erythrodysesthesia; radiation recall urticaria, exanthems, mucositis, alopecia, nail changes (see Section 32); scleroderma-like changes on lower extremities; subacute cutaneous lupus erythematosus (SCLE), AGEP and fixed drug reaction (paclitaxel) Vinca alkaloids: vincristine, vinblastine, vinorelbine
Phlebitis, alopecia, acral erythema, extravasation reactions (including necrosis)
Antimetabolites Fludarabine Serpentine supravenous hyperpigmentation, macular, papular exanthem, mucositis, acral erythema, paraneoplastic pemphigus, drug-induced SCLE Cladribine Exanthem, TEN, exfoliative dermatitis Capecitabine Hand–foot skin reactionb acral hyperpigmentation, palmoplantar keratoderma, pyogenic granuloma, inflammation of actinic keratoses Tegafur Hand–foot skin reactionb acral hyperpigmentation; pityriasis lichenoides et varioliformis acuta, phototoxic reactions Gemcitabine Mucositis, alopecia, maculopapular exanthem, radiation recall, linear IgA bullous dermatosis, pseudoscleroderma, lipodermatosclerosis, erysipelas-like plaques, pseudolymphoma, lymphomatoid papulosis Pemetrexed Exanthema, radiation recall, urticarial vasculitis
Genotoxic agents Carboplatin Alopecia, hypersensitivity reaction (erythema, facial swelling, dyspnea, tachycardia, wheezing), palmoplantar erythema, facial flushing Oxaliplatin Hypersensitivity reaction (see preceding); irritant extravasation reaction; radiation recall Liposomal doxorubicin Acral erythema, palmoplantar erythrodysesthesia neutrophilic eccrine hidradenitis, hyperpigmentation (blue-gray), mucositis, alopecia, exanthems, radiation recall, ultraviolet light recall Liposomal daunorubicin Alopecia, mucositis, extravasation reactions Idarubicin Radiation recall; alopecia, acral erythema, mucositis, nail changes (transverse pigmented bands), extravasation reactions Topotecan Maculopapular exanthem, alopecia, neutrophilic hidradenitis Irinotecan Mucositis, alopecia, lichenoid reactions
Signal transduction inhibitors EGFR antagonists: gefitinib, cetuximab, erlotinib, panitumumab
Papulopustular eruptions in seborrheic areas, erythematous plaques, telangiectasias; xerosis, paronychia; hair abnormalities (trichomegaly, curling, fragility, see Section 31) Usually start a week after initiation of drug. Can treat with topical antibiotics, retinoids (topical or systemic). Can also lead to paronychia (Fig. 23-18A), trichomegaly (Fig. 23-18B), leukocytoclastic vasculitis, urticaria, anaphylaxis, and necrolytic migratory erythema.
(continued)
Class Agents ACDRa
Multikinase inhibitors: Imatinib Maculopapular exanthem (face, forearms, ankles), exfoliative dermatitis, graft-versus-host reaction-like reaction, erythema nodosum, vasculitis, SJS, AGEP; hypopigmentation, hyperpigmentation, darkening of hair, nail hyperpigmentation, lichen planus-like eruption (skin and oral mucosa), follicular mucinosis, pityriasis rosealike eruption, Sweet syndrome, exacerbation of psoriasis, palmoplantar hyperkeratosis, porphyria cutanea tarda, primary cutaneous EBV-related B-cell lymphoma Dasatinib and nilotinib Localized and generalized erythema, maculopapular exanthem, mucositis, pruritus, exfoliation, alopecia, xerosis “acne,” urticaria, panniculitis, Sweet syndrome. Sorafenib and sunitinib Rash/desquamation, hand-foot skin reactionb pain, alopecia, mucositis, xerosis, flushing edema, seborrheic dermatitis, yellow skin coloration (sunitinib, 1 week after starting drug), subungual splinter hemorrhages, pyoderma gangrenosum, SCC (KA-type) and eruptive melanocytic lesions (sorafenib)
Proteasome inhibitor Immune Modulators
Bortezomib Ipilimumab (CTLA-4 AB) Pembrolizumab and Nivolumab (PD-1 receptor antibody) Vemurafenib Dabrafenib
Erythematous nodules and plaques, morbilliform exanthem, ulceration, vasculitis and Sweet syndrome Immune-mediated side effects: macular and papular eruption, pruritus, hepatitis, vitiligo, hypothyroidism, enterocolitis, hepatitis, SJS/TEN Immune-mediated side effects: macular and papular eruption (Fig. 23-19A), pruritus, vitiligo, hypothyroidism, enterocolitis, hepatitis, mucositis (Fig. 23-19B). Rash (68%), arthralgias, photosensitivity (42%), SCC (23%, most occur in first few months) Pyrexia, headaches, rash
BRAF inhibitors
aOnly cutaneous adverse reactions are listed here.
bHand–foot skin reaction: erythema, hyperkeratotic with halo of erythema, tender, localized to areas of pressure on fingertips, toes, and heels. Source: Collated from Haidary N et al. J Am Acad Dermatol. 2008;58:545. Please note that this table has also been supplemented by the authors.
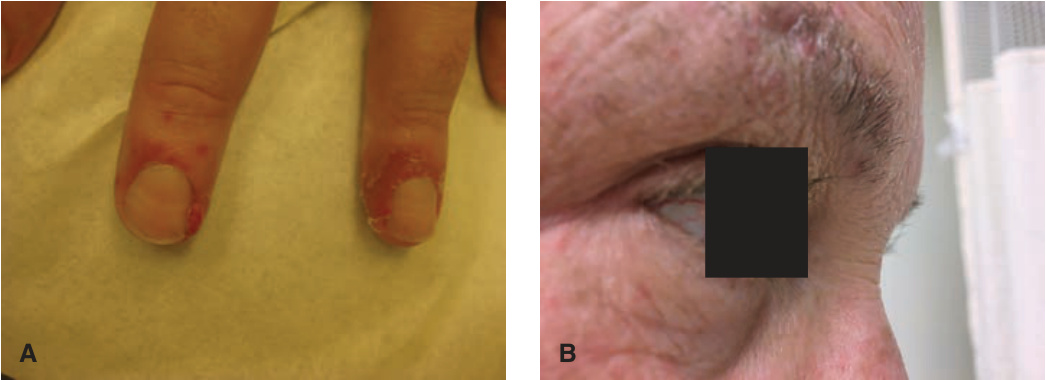
FIGURE 23-18 • ACDR to EGFR antagonists: erlotinib (A) Periungal erythema and scaling, commonly seen in drug-induced paronychia. (B) Trichomegaly. The patient complained of this during an examination for skin cancer surveillance.
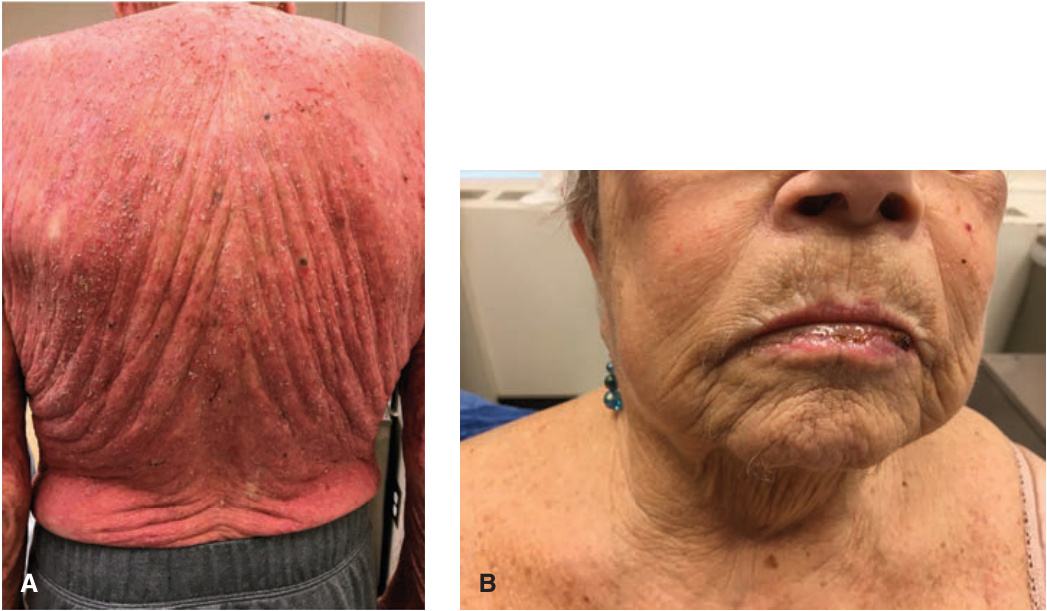
FIGURE 23-19 • ACDR to Immune modulators (A) Confluent macular and papular exanthema over an erythematous background in a patient treated with pembrolizumab. (B) Mucositis can be a difficult symptom to treat. Erosions are noted along the entire length of the lower lip.
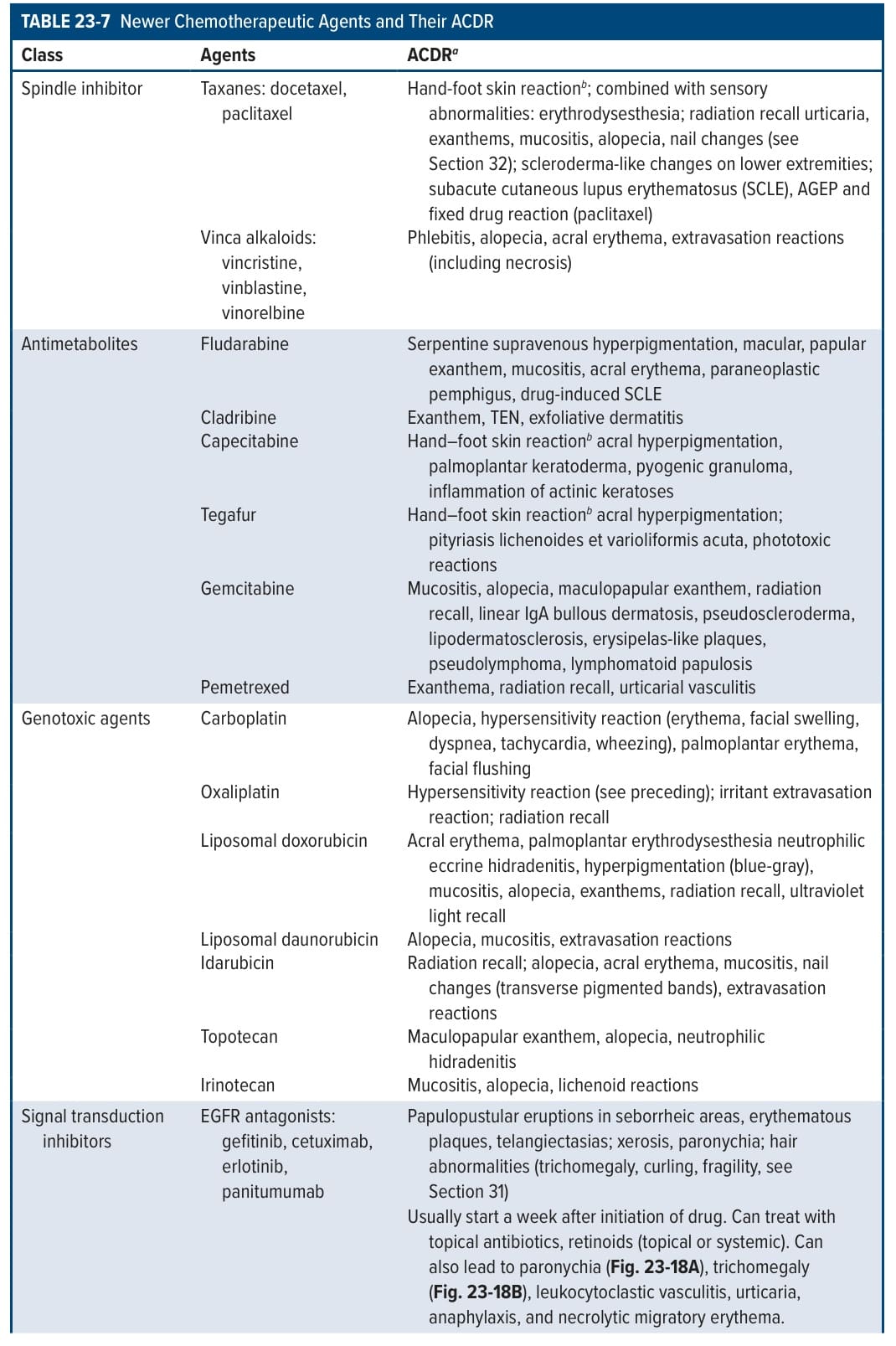
TABLE 23-7 Newer Chemotherapeutic Agents and Their ACDR