ERYTHRASMA
ERYTHRASMA ICD-10: L08.1
• Etiology. Corynebacterium minutissimum, gram-positive (diphtheroid) bacillus; normally in human microbiome. Growth favored by humid cutaneous microclimate.
CLINICAL MANIFESTATION
Most often asymptomatic, although pruritus may be present. Subtle discoloration. Patches, sharply marginated (Fig. 25-1). Tan or pinkish; postinflammatory
hyperpigmentation in more heavily pigmented individuals. In webspaces of the feet, it may be macerated (Fig. 25-2). Distribution: Intertriginous skin, i.e., toe webs (Fig. 25-2), inguinal folds, axillae, and other occluded sites.
DIAGNOSIS
Wood’s lamp examination demonstrates corral-red fluorescence. KOH negative; rules out epidermal dermatophytosis.
DIFFERENTIAL DIAGNOSIS
Intertriginous psoriasis, epidermal dermatophytosis, pityriasis versicolor, and Hailey– Hailey disease.
COURSE
Persists and recurs unless microclimate is altered.
TREATMENT
Usually controlled with benzoyl peroxide wash or sanitizing alcohol gel. Clindamycin lotion and erythromycin are beneficial.
A B

FIGURE 25-1 • Erythrasma: Groins Sharply marginated, tan patches in the genitocrural fold. Wood lamps demonstrates bright coral-red fluorescence differentiating erythrasma from intertriginous psoriasis. KOH preparation was negative for hyphae.
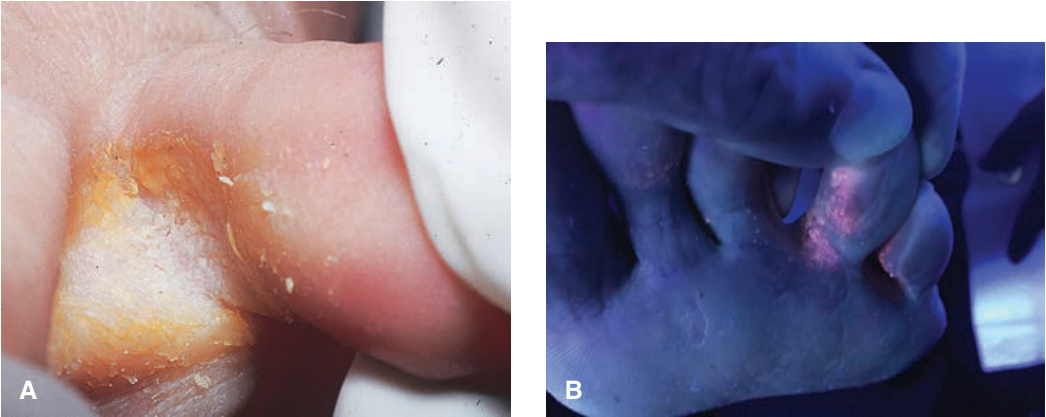
FIGURE 25-2 • A, B Erythrasma: Webspace This macerated interdigital webspace appeared bright coral-red when examined with Wood’s lamp; KOH preparation was negative for hyphae. The webspace is the most common site for erythrasma in temperate climates. In some cases, interdigital tinea pedis and/or pseudomonal intertrigo may coexist.