PITTED KERATOLYSIS
PITTED KERATOLYSIS
• Etiology. Kytococcus sedentarius. One of human microbiome on plantar feet in the setting of hyperhidrosis; produces two extracellular proteases that can digest keratin.
CLINICAL MANIFESTATION
Punched out pits in stratum corneum, 1 to 8 mm in diameter (Fig. 25-3A and B). Pits can remain discrete or become confluent, forming large areas of eroded stratum corneum. Lesions are more apparent with hyperhidrosis and maceration. Symmetric or asymmetric involvement of both feet. Distribution: Pressure-bearing areas, ventral aspect of toe, ball of foot, heel; interface of toes.
DIAGNOSIS
Clinical diagnosis. KOH to rule out tinea pedis.
DIFFERENTIAL DIAGNOSIS
Concomitant tinea pedis, erythrasma, candidal intertrigo, and pseudomonal webspace infection may be present.
COURSE
Persists and recurs unless microclimate is altered.
TREATMENT
Usually controlled with benzoyl peroxide wash or sanitizing alcohol gel. Topical antibiotics, such as erythromycin and clindamycin, and aluminum chloride solution can also be helpful.
A B
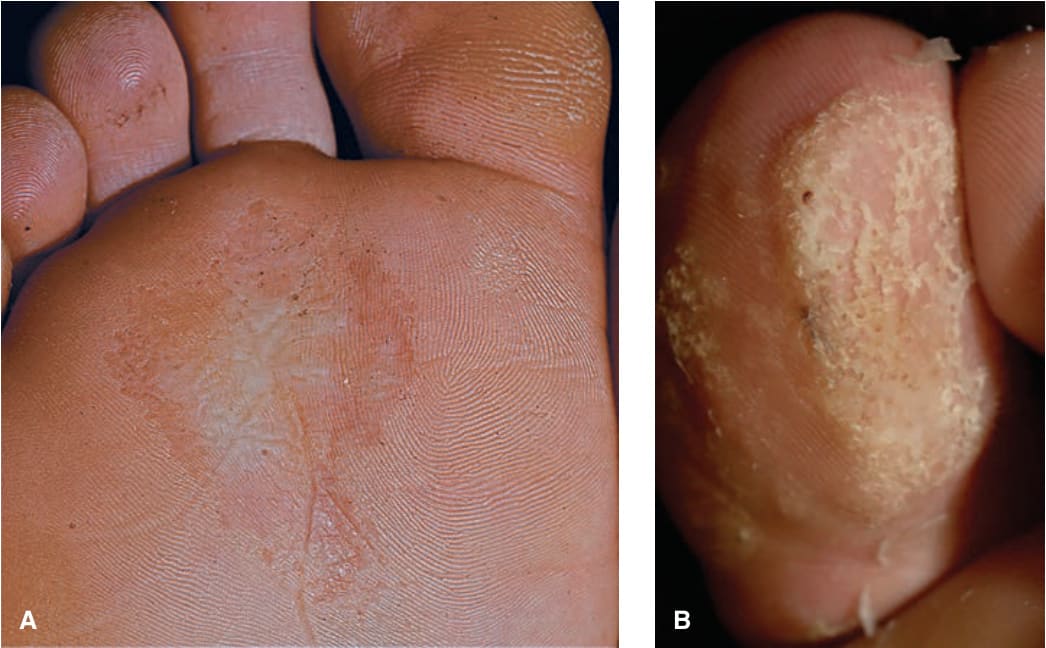
FIGURE 25-3 • A, B Pitted keratolysis: Plantar The stratum corneum of the plantar skin (A) and toe-pad (B) shows confluent multiple, confluent “pits” (defects in the stratum corneum).