CELLULITIS
CELLULITIS ICD-10: A46.0
• Acute, spreading infection of dermal and subcutaneous tissues. Characterized by a red, hot, and tender area of skin. Portal of entry of infection is usually apparent. Most common pathogen is S. aureus. Erysipelas is a variant of cellulitis involving cutaneous lymphatics, and is usually caused by beta-hemolytic streptococci.
EPIDEMIOLOGY AND ETIOLOGY
ETIOLOGY Adults: S. aureus, GAS. Less commonly beta-homolytic streptococcus: Group B, C, or G. Erysipelothrix rhusiopathiae (erysipeloid); P. aeruginosa, Pasteurella multocida, Vibrio vulnificus; Mycobacterium fortuitum complex. In children: Pneumococci, Neisseria meningitidis group B (periorbital). Haemophilus influenzae type b (Hib) infections much less common because of Hib immunization. Chronic Soft-Tissue Infections. Nocardia brasiliensis, Sporothrix schenckii, Madurella species, Scedosporium species, and nontuberculous mycobacteria (NTM). Dog and Cat Saliva and Bites: P. multocida and other Pasteurella species. Capnocytophaga canimorsus (see Septic shock: Ischemic necrosis of acral sites, p. 591). PORTAL OF INFECTION Pathogens gain entry via any break in the skin or mucosa. Tinea pedis and leg and foot ulcers are common portals. Infections follow bacteremia/sepsis with cutaneous seeding. RISK FACTORS Host defense defects, diabetes mellitus, drug and alcohol abuse, cancer and cancer
chemotherapy, chronic lymphedema (postmastectomy, previous episode of cellulitis/erysipelas). After entry, infection spreads to tissue spaces and cleavage planes (Fig. 25-25) as hyaluronidases break down polysaccharide ground substances, fibrinolysins digest fibrin barriers, and lecithinases destroy cell membranes. Local tissue devitalization is usually required to allow for significant anaerobic bacterial infection. The number of infecting organisms is usually small, suggesting that cellulitis may be more of a reaction to cytokines and bacterial superantigens than to overwhelming tissue infection.
CLINICAL MANIFESTATION
Symptoms of fever and chills can develop before cellulitis is clinically apparent. Higher fever (38.5°C) and chills usually associated with GAS infection. Local pain and tenderness. Necrotizing infections associated with severe pain and systemic symptoms. Red, hot, edematous, and shiny plaque originating at the portal of entry. Enlarges with proximal extension (Figs. 25-26 and 25-27);
Crust Eschar
Epidermis
Dermal papillae
Postcapillary venule
Subcutaneous fat
Deep fascia
Bulla
Erysipelas
Cellutitis
Necrotizing fasciitis Lymphatic channel
Vein
Artery
Muscle Myositis
Bone
A B
A B
borders are irregular, slightly elevated and fade leaving a “sunset” sign. Vesicles, bullae, erosions, abscesses, hemorrhage, and necrosis may form in plaque (Fig. 25-27A and B). Lymphangitis. Lymph nodes can be enlarged and tender regionally. DISTRIBUTION Adults. Lower extremity is the most common site (Fig. 25-27). Arm: In young male, consider IV drug use; in female, postmastectomy (Fig. 25-28). Trunk: Operative wound site. Face: Following rhinitis, conjunctivitis, pharyngitis; associated with colonization of nares by S. aureus and of pharynx by GAS.
VARIANTS OF CELLULITIS BY PATHOGEN
S. aureus: Portal of entry is usually apparent; cellulitis is an extension of focal infection. Toxin syndromes: Scalded-skin syndrome, TSS. Endocarditis may follow bacteremia.
Beta-hemolytic streptococci GAS (Streptococcus pyogenes) colonize skin and oropharynx. GBS and GGS colonize anogenital region. Beta-hemolytic streptococcal soft-tissue infections spread rapidly along superficial cutaneous lymphatic vessels, presenting tender red expanding plaques, i.e., erysipelas (Figs. 25-29 and 25-30). Following childbirth, known as puerperal sepsis; infection can extend into pelvis. GBS cellulitis occurs in neonates; high morbidity and mortality. GAS infection with necrotizing fasciitis and streptococcal TSS has high morbidity and mortality. E. rhusiopathiae: Erysipeloid occurs in individuals who handle swine, sheep, poultry, or fish. Painful, inflamed plaque with sharply defined irregular raised border occurring at the site of inoculation, i.e., the fingers or hand (Fig. 25-31), spreading to the wrist but
A B
not to forearm. Color: Purplish red acutely; brownish with resolution. Enlarges peripherally with central fading. Usually no systemic symptoms. Ecthyma gangrenosum: Rare variant of necrotizing soft-tissue infection caused by P. aeruginosa in ill patients. Clinically characterized by infarcted center with erythematous halo, expanding rapidly without effective treatment (Fig. 25-32). Distribution: Most commonly in the axilla, groin, or perineum. Prognosis depends on prompt diagnosis, treatment, and restoration of host defense defects, usually correction of neutropenia. H. influenzae: Occurs mainly in children <2 years. Cheek, periorbital area, head, and neck are most common sites. Clinically, swelling, characteristic violaceous erythema hue. Use of Hib vaccine has dramatically reduced incidence. V. vulnificus, V. cholerae non-01 and non-
0139. Underlying disorders: Cirrhosis, diabetes, immunosuppression, hemochromatosis, and thalassemia. Follows ingestion of raw/ undercooked seafood, gastroenteritis, bacteremia with seeding of skin; also exposure of skin to seawater. Characterized by bulla formation,
necrotizing vasculitis (Fig. 25-33). Usually on the extremities; often bilateral. Aeromonas hydrophila: Water-associated trauma; preexisting wound. Immunocompromised host. Lower leg. Necrotizing soft-tissue infection. C. canimorsus. Immunosuppression or asplenia; exposure to dog saliva or bite. Causes fulminant sepsis and disseminated intravascular coagulation (see Septic shock: Ischemic necrosis of acral sites, p. 591). P. multocida: Most common cause of infection following animal bite; soft-tissue infection. Clostridium species. Associated with trauma; contamination by soil or feces; malignant intestinal tumor. Infection characterized by gas production (crepitation on palpation), marked systemic toxicity. Necrotizing infection. Nontuberculous mycobacteria. History of recent surgery, injection, penetrating wound, systemic corticosteroid therapy. Low-grade cellulitis. Multiple sites of infection. Systemic findings lacking. Cryptococcus neoformans: Immunocompromised. Red, hot, tender, edematous plaque on extremity. Rarely multiple noncontiguous sites.
Mucormycosis: Usually occurring in individuals with uncontrolled diabetes. Nocardiosis: See Cutaneous Nocardia Infections, p. 583. Eumycetoma: See Section 26. Chromoblastomycosis: See Section 26.
DIFFERENTIAL DIAGNOSIS
ERYSIPELAS/CELLULITIS Deep vein thrombophlebitis, urticaria, insect bite (hypersensitivity response), fixed drug eruption, erythema nodosum, acute gout, and erythema migrans (EM). NECROTIZING STIs Vasculitis, occlusive vasculopathy, peripheral vascular disease, calciphylaxis, warfarin necrosis, traumatic injury, cryoglobulinemia, pyoderma gangrenosum, and brown recluse spider bite.
DIAGNOSIS
Clinical diagnosis is based on morphologic features of lesion and the clinical setting, i.e., underlying diseases, travel history, animal
exposure, history of bite, and age. Confirmed by culture in only 29% of cases in immunocompetent patients. Suspicion of necrotizing fasciitis (see below) requires immediate deep biopsy and tissue culture.
COURSE
With timely diagnosis and treatment, soft-tissue infection resolves with oral or parenteral antibiotic treatment. Dissemination of infection (lymphatics, hematogenously), with metastatic sites of infection occurring, if effective treatment is delayed. In immunocompromised patients, prognosis depends on prompt restoration of altered immunity, usually on correction of neutropenia.
TREATMENT
Systemic high-dose antibiotic treatment according to type and sensitivity of microbial organism.
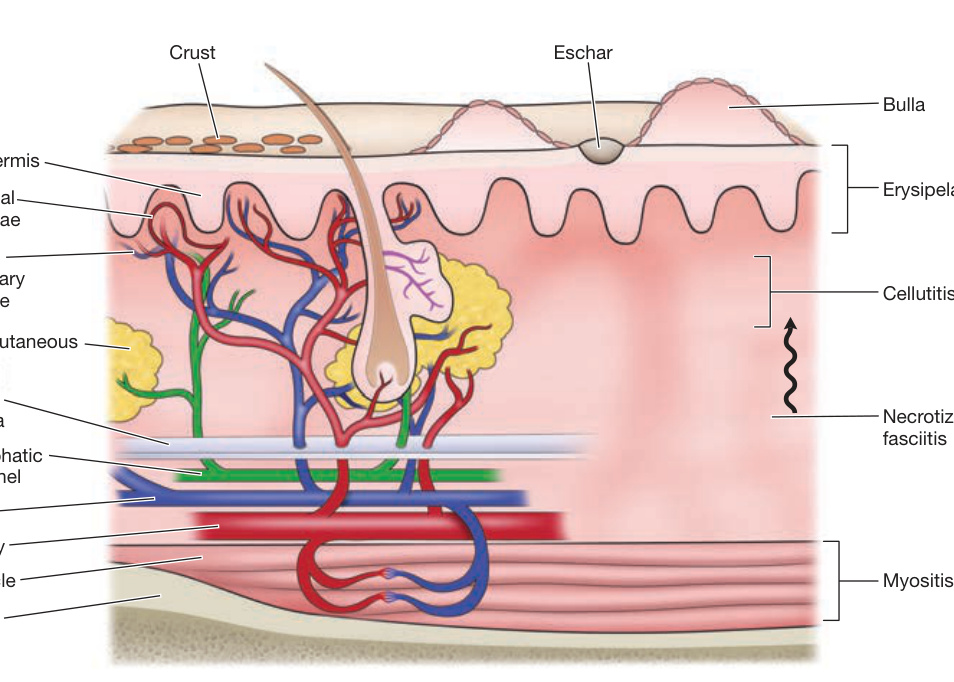
FIGURE 25-25 • Structural components of the skin and soft tissue, superficial infections, and infections of the deeper structures The rich capillary network beneath the dermal papillae plays a key role in the localization of infection and in the development of the acute inflammatory reaction. (Reproduced with permission from Stevens DL. Infections of the skin, muscles, and soft tissues. In: Longo DL, Fauci AS, Kasper DL, et al., eds. Harrison’s Principles of Internal Medicine. 18th ed. New York, NY: McGraw Hill; 2012.)
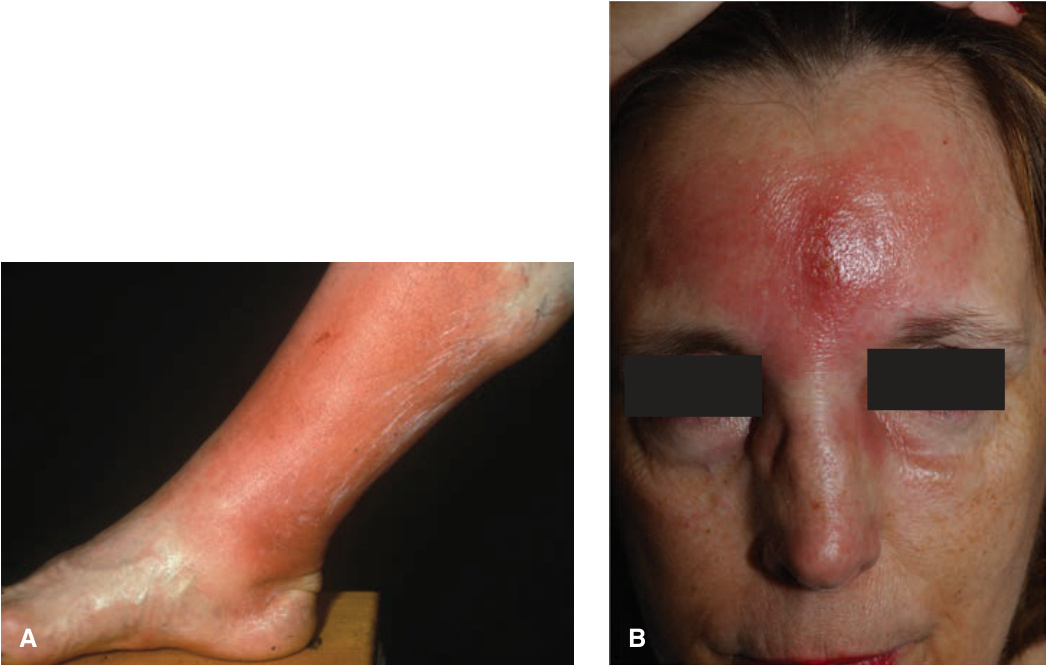
FIGURE 25-26 • Cellulitis at portal of entry: MSSA (A) A 51-year-old male with a warm, red, edematous and tender right leg. Methicillin-sensitive S. aureus was isolated on culture of the first webspace. (B) A 52-year-old woman with tender, red, warm and edematous plaque of central forehead. Infection developed after excoriation of an acneiform pustule.

FIGURE 25-27 • Cellulitis with necrosis: MRSA (A) A 70-year-old man with increasing erythema and edema of the left lateral leg associated with fever. Early dusky discoloration noted proximally. (B) A 61-year-old woman with cellulitis of the right buttock and central necrosis. She was febrile and had severe pain overlying the infection.

FIGURE 25-28 • Recurrent cellulitis of the arm with chronic lymphedema: MSSA Right breast cancer had been treated with mastectomy and lymph node excision 10 years previously. Lymphedema of the right arm followed. Hand dermatitis was secondarily infected with MSSA. Cellulitis occurred repeatedly in the setting of chronic lymphedema.

FIGURE 25-29 • Erysipelas of thigh: Group B streptococcus A 52-year-old woman with fever. Portal of entry was an insect bite in the popliteal fold. Lesion was very painful.
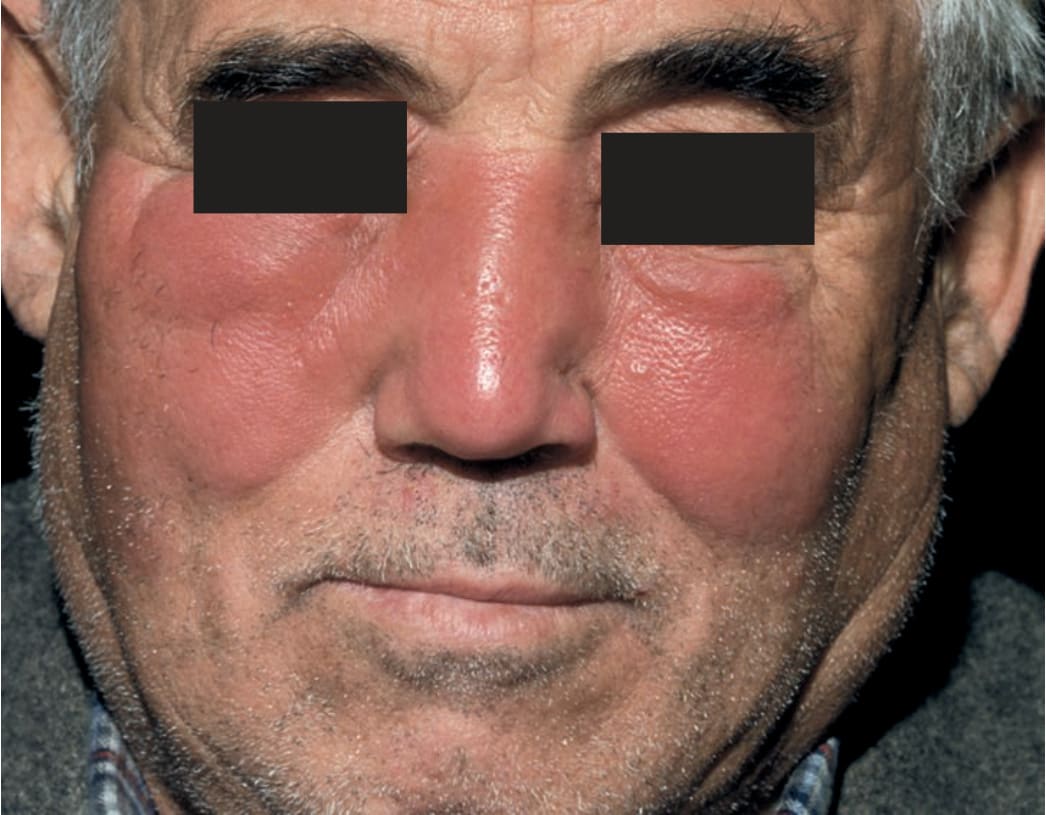
FIGURE 25-30 • Erysipelas of face: Group A streptococcus Painful, well-defined, shiny, erythematous, edematous plaques involving the central face of an otherwise healthy man. On palpation, the skin is hot and tender. There is fever (39.5°C).

FIGURE 25-31 • Erysipeloid of hand A well-demarcated, violaceous, edematous plaque (without epidermal changes of scale or vesiculation) on the dorsa of the hand and fingers, occurred following cleaning fish; the site was somewhat painful, tender, and warm.
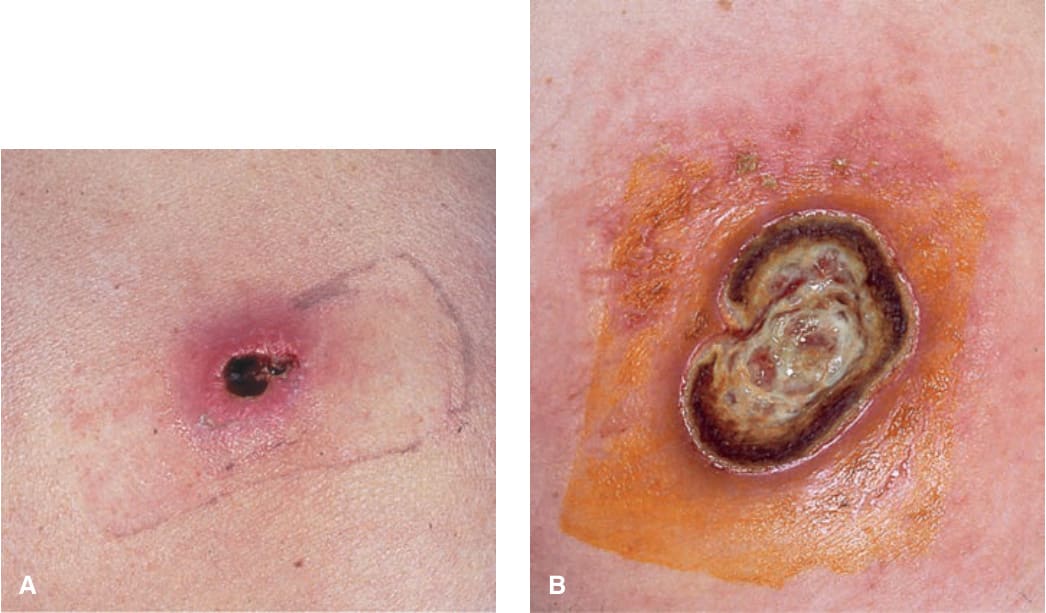
FIGURE 25-32 • Ecthyma gangrenosum of buttock: P. aeruginosa A 30-year-old male with HIV disease and neutropenia. (A) An extremely painful, infarcted area with surrounding erythema present for 5 days. This primary cutaneous infection was associated with bacteremia. (B) Two weeks later, the lesion had progressed to a large ulceration. The patient died 3 months later of P. aeruginosa pneumonitis associated with chronic neutropenia.

FIGURE 25-33 • Bilateral cellulitis of legs: V. vulnificus Bilateral hemorrhagic plaques and bullae on the legs, ankles, and feet of an older diabetic with cirrhosis. Unlike other types of cellulitis in which microorganisms enter the skin locally, this type of cellulitis (caused by V. vulnificus) usually follows a primary enteritis with bacteremia and subsequent dissemination to the skin. However, most cases initially diagnosed as bilateral cellulitis are inflammatory (eczema, stasis dermatitis, psoriasis) rather than infectious.