CAT-SCRATCH DISEASE (CSD)
CAT-SCRATCH DISEASE (CSD) ICD-10: A28.1
• Etiology. B. henselae. Reservoir: Domestic cat.
• Transmission. Associated with exposure to young cats. Blood cultures of kittens are frequently positive for B. henselae. Cat flea Ctenocephalides felis transmit infection between cats.
• Demography/Age of Onset. Majority of cases occur in children.
• Pathogenesis. B. henselae causes granulomatous inflammation in healthy individuals (CSD) and angiogenesis in immunocompromised persons.
CLINICAL MANIFESTATION
INOCULATION SITE Innocuous-looking, small (0.5 to 1 cm) papule, vesicle, or pustule; may ulcerate; skin color pink to red; firm, at times tender (Fig. 25-60). Residual linear cat scratch. Persists for 1 to 3 weeks. Distribution: Exposed skin of the face and hands. CONJUNCTIVAE If portal of entry is the conjunctiva, 3- to 5-mm whitish-yellow granulation on palpebral conjunctiva associated with tender preauricular and/or cervical lymphadenopathy (Parinaud oculoglandular syndrome). Uncommonly urticaria, transient maculopapular eruption, or erythema nodosum. REGIONAL LYMPHADENOPATHY (Fig. 25-61) Evident within 2 to 3 weeks after inoculation in 90% of cases; primary lesion, if present, may have resolved by the time lymphadenopathy occurs. Nodes are often solitary, moderately tender, and freely movable. Involved lymph nodes: Epitrochlear, axillary, pectoral, and cervical. Nodes may suppurate.
Usually resolved within 3 months. Generalized lymphadenopathy or involvement of the lymph nodes of more than one region is unusual.
DIFFERENTIAL DIAGNOSIS
Chancriform syndrome. Suppurative bacterial lymphadenitis, NTM infection, sporotrichosis, and tularemia. OTHER CAT-ASSOCIATED INFECTIONS Bite infections caused by P. multocida and C. canimorsus, sporotrichosis; Microsporum canis dermatophytosis.
DIAGNOSIS
Suggested by regional lymphadenopathy developing over 2 to 3 weeks in an individual with cat contact and a primary lesion at the site of contact; confirmed by identification of B. henselae from tissue or serodiagnosis.
COURSE
Self-limiting, usually within 1 to 2 months. Uncommonly, prolonged morbidity with persistent high fever, suppurative lymphadenitis,
and severe systemic symptoms. May be confused with lymphoma. Uncommonly, cat-scratch encephalopathy occurs. Antibiotic therapy has not been very effective in altering the course of the infection.
TREATMENT
In the immunocompromised, azithromycin; in immunocompetent, spontaneous resolution occurs.
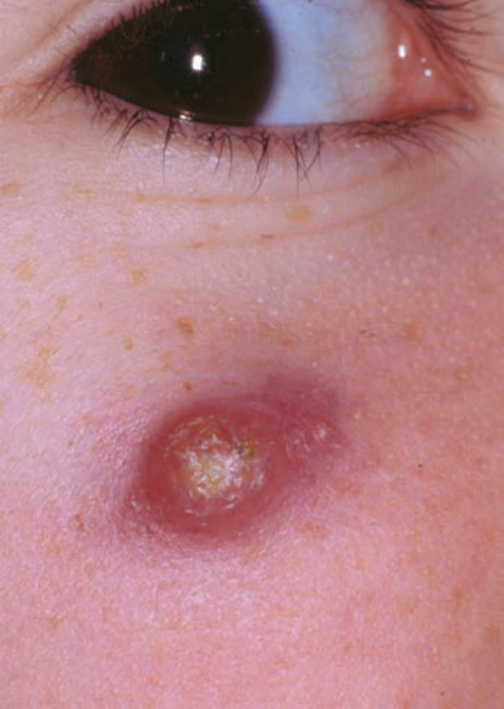
FIGURE 25-60 • Bartonellosis: Cat-scratch disease with primary lesion Erythematous nodule of the cheek of a 9-year-old girl at the site of cat scratch. Diagnosis was made on the histologic findings of the excised specimen.

FIGURE 25-61 • Bartonellosis: Cat-scratch disease with axillary adenopathy Acute, very tender, axillary lymphadenopathy in a child; cat scratches were present on the dorsum of the ipsilateral hand. (Used with permission from Howard Heller, MD.)