TULAREMIA
TULAREMIA ICD-10: A21
• Etiology: Francisella tularensis, types A and B. After inoculation into skin, mucous membrane, lung (inhalation), or GI tract, F. tularensis reproduces and spreads through lymphatic channels to the lymph nodes and bloodstream.
• Transmission. Bite of insect vector (ticks, deer flies, body lice, or other arthropods). Handling flesh of infected animals; inoculation of conjunctiva; ingestion of infected food; inhalation. Most U.S. cases occur in June to September when arthropod transmission is most common.
• Animal Reservoir. Rabbits, hares, muskrats, squirrels, voles, and beavers.
• Incidence. Rare; <200 cases reported in the United States per year; underdiagnosed, underreported.
CLINICAL MANIFESTATION
About 48 hours after inoculation, pruritic papule develops at the site of trauma or insect bite followed by enlargement of the regional lymph nodes. Fever to 41°C. Inoculation site: Erythematous tender papule evolving to a vesicopustule, enlarging to crusted ulcer with raised, sharply demarcated margins (96 hours) (Fig. 25-63). Depressed center that is often covered by a black eschar (chancriform). Primary lesion on the finger or hand at the site of trauma or insect bite; groin or axilla after tick bite. OTHER CUTANEOUS FINDINGS Exanthem may occur after bacteremia on the trunk and extremities with macules, papules, and petechiae. Erythema multiforme. Erythema nodosum. CONJUNCTIVAE In oculoglandular tularemia, F. tularensis is inoculated into conjunctiva, causing a purulent conjunctivitis with pain, edema, and congestion. Small yellow nodules occur on conjunctivae and ulcerate. REGIONAL LYMPH NODES As the ulcer develops, nodes enlarge and become tender, i.e., chancriform syndrome (Fig. 25-63). If untreated, they become suppurating buboes.
DIFFERENTIAL DIAGNOSIS
Acute cutaneous ulcer: Furuncle, paronychia, anthrax, P. multocida infection, sporotrichosis, and M. marinum infection. Chancriform syndrome: Herpes simplex virus lymphadenitis, plague, and cat-scratch disease.
DIAGNOSIS
Clinical diagnosis in a patient with chancriform syndrome with appropriate animal or insect exposure.
COURSE
Untreated, mortality rate for ulceroglandular form is 5%; 1% if therapy is initiated promptly.
TREATMENT
Streptomycin is the treatment of choice. Also gentamycin, chloramphenicol, doxycycline, and ciprofloxacin.
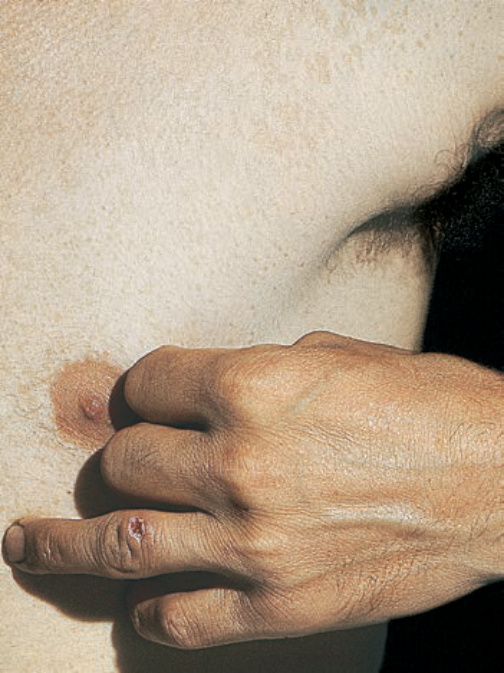
FIGURE 25-63 • Tularemia: Primary lesion and regional adenopathy A crusted ulcer at the site of inoculation is seen on the dorsum of the left ring finger with associated axillary lymph node enlargement (chancriform syndrome). The infection occurred after the patient killed and skinned a rabbit.