HANSEN DISEASE (LEPROSY)
HANSEN DISEASE (LEPROSY) ICD-10: A30
• Etiology. Mycobacterium leprae.
• Chronic granulomatous disease principally acquired during childhood or young adulthood.
• Sites of infection. Skin, peripheral nervous system, upper respiratory tract, eyes, and testes.
• Clinical manifestations, natural history, and prognosis of leprosy are related to the host response: Various types of leprosy (tuberculoid, lepromatous, etc.) represent the spectra of the host’s immunologic response (cell-mediated immunity).
Source: https://www.cdc.gov/leprosy/index.html.
CLASSIFICATION
Based on clinical, immunologic, and bacteriologic findings.
• Tuberculoid (TL): Localized skin involvement and/or peripheral nerve involvement; few organisms.
• Lepromatous (LL): Generalized involvement including skin, upper respiratory mucous membrane, reticuloendothelial system, adrenal glands, and testes; many bacilli.
• Borderline (or “dimorphic”) (BL): Has features of both TL and LL. Usually many bacilli present, varied skin lesions: macules, plaques; progresses to TL or regresses to LL.
• Indeterminate forms.
• Transitional forms: See “Pathogenesis,” in the following discussion.
ETIOLOGY AND EPIDEMIOLOGY
Mycobacterium leprae: Obligate intracellular acid-fast bacillus; reproduces optimally at 27°C to 30°C. Organism cannot be cultured in vitro. Infects skin and cutaneous nerves (Schwann cell basal lamina). In untreated
patients, only 1% of organisms are viable. Grows best in cooler tissues (skin, peripheral nerves, anterior chamber of eye, upper respiratory tract, and testes), sparing warmer areas of the skin (axilla, groin, scalp, and midline of back). Humans are main reservoirs of M. leprae. Wild armadillos (southern United States) as well as mangabey monkeys and chimpanzees are naturally infected with M. leprae; armadillos can develop lepromatous lesions. Incidence rate peaks at 10 to 20 years; prevalence peaks at 30 to 50 years. More common in males than in females. Inverse relationship between skin color and severity of disease; in black Africans, susceptibility is high, but there is predominance of milder forms of the disease, i.e., TL vis-à-vis LL. TRANSMISSION Uncertain. Likely spread from person to person in respiratory droplets. DEMOGRAPHY Disease of the developing world. In 2020, 127,558 new cases were reported worldwide to the World Health Organization, with the most in Southeast Asia. Risk groups: Close contact with patients with untreated,
active, predominantly multibacillary disease, and persons living in countries with highly endemic disease. Most individuals have natural immunity and do not develop disease. PATHOGENESIS Clinical spectrum of leprosy depends exclusively on variable limitations in host’s capability to develop effective cell-mediated immunity to M. leprae. Organism is capable of invading and multiplying in peripheral nerves and infecting and surviving in endothelial and phagocytic cells in many organs. Subclinical infection with leprosy is common among residents in endemic areas. Clinical expression of leprosy is development of a granuloma; patient may develop a “reactional state,” which may occur in some form in >50% of certain groups of patients.
GRANULOMATOUS SPECTRUM OF LEPROSY
• High-resistance tuberculoid response (TT).
• Low- or absent-resistance lepromatous pole (LL).
• Dimorphic or borderline region (BB).
• Two intermediary regions.
• Borderline lepromatous (BL).
• Borderline tuberculoid (BT).
In order of decreasing resistance, the spectrum is TT, BT, BB, BL, and LL. IMMUNOLOGIC RESPONSES Immune responses to M. leprae can produce several types of reactions associated with a sudden change in the clinical status. Lepra Type 1 Reactions. Acute or insidious tenderness and pain along affected nerve(s), associated with loss of function. Lepra Type 2 Reactions. Erythema nodosum leprosum (ENL). Seen in half of LL patients, usually occurring after initiation of antilepromatous therapy, generally within the first 2 years of treatment. Massive inflammation with erythema nodosum–like lesions. Lucio Reaction. Individuals with diffuse LL develop shallow, large polygonal sloughing ulcerations on the legs. The reaction appears to be either a variant of ENL or secondary to arteriolar occlusion.
CLINICAL MANIFESTATION
Incubation period is 2 to 40 years (most commonly 5 to 7 years). Onset is insidious and painless; first affects peripheral nervous
system with persistent or recurrent painful paresthesias and numbness without any visible clinical signs. At this stage, there may be transient macular skin eruptions; blister, but lack of awareness of trauma. Neural involvement leads to muscle weakness, muscle atrophy, severe pain, and contractures of the hands and feet. TUBERCULOID LEPROSY (TT, BT) Few well-defined hypopigmented hypoesthetic macules (Fig. 25-64) with raised edges and varying in size from a few millimeters to very large lesions covering the entire trunk. Erythematous or purple border and hypopigmented center. Sharply defined, raised; often annular; enlarge peripherally. Central area becomes atrophic or depressed. Advanced lesions are anesthetic, devoid of skin appendages (sweat glands or hair follicles). Any site including the face. TT: Lesions may resolve spontaneously; not associated with lepra reactions. BT: Does not heal spontaneously; type 1 lepra reactions may occur. Nerve Involvement: May be a thickened nerve on the edge of the lesion; large peripheral nerve enlargement frequent (ulnar, posterior auricular, peroneal, and posterior tibial nerves). Skin involvement is absent in neural leprosy. Nerve involvement is associated with hypesthesia (pinprick, temperature, or vibration) and myopathy. BORDERLINE BB LEPROSY Lesions are intermediate between tuberculoid and lepromatous and are composed of macules, papules, and plaques (Fig. 25-65). Anesthesia and decreased sweating are prominent in the lesions. LEPROMATOUS LEPROSY (LL, BL) Skin-colored or slightly erythematous papules or nodules. Lesions enlarge; new lesions occur and coalesce. Later, symmetrically distributed nodules, raised plaques, diffuse dermal infiltrate, which on the face results in loss of hair (lateral eyebrows and eyelashes) and leonine facies (lion’s face; Fig. 25-66). Diffuse lepromatosis, occurring in western Mexico, Caribbean, presents as diffuse dermal infiltration and thickened dermis. Bilaterally symmetric involving the earlobes, face, arms, and buttocks, or less frequently the trunk and lower extremities. Tongue: Nodules, plaques, or fissures.
Nerve Involvement: More extensive than in TT. Other Involvement: Upper respiratory tract, anterior chamber of eye, and testes.
Reactional States Immunologically mediated inflammatory states, occurring spontaneously or after initiation of therapy. Lepra Type 1 Reactions: Skin lesions become acutely inflamed, associated with edema
and pain; may ulcerate. Edema is most severe on the face, hands, and feet. Lepra Type 2 Reactions (ENL): Present as painful red skin nodules arising superficially and deeply. In contrast the true erythema nodosum lesions form abscesses or ulcerate; they occur most commonly on the face and extensor limbs. Lucio Reaction: Occurs in patients from Mexico or Caribbean with diffuse LL. Presents as irregularly shaped erythematous plaques;
lesions may resolve spontaneously or undergo necrosis with ulceration.
General Findings Extremities: Sensory neuropathy, plantar ulcers, secondary infection; ulnar and peroneal palsies (Fig. 25-67), Charcot joints. Squamous cell carcinoma can arise in chronic foot ulcers. Nose: Chronic nasal congestion, epistaxis; destruction of cartilage with saddle-nose deformity (Fig. 25-67). Eyes: Cranial nerve palsies, lagophthalmos, and corneal insensitivity. In LL, anterior
chamber can be invaded with uveitis, glaucoma, and cataract formation. Corneal damage can occur secondary to trichiasis and sensory neuropathy, secondary infection, and muscle paralysis. Testes: May be involved in LL with resultant hypogonadism. Complications of Leprosy: Squamous cell carcinoma can arise in chronic neurotrophic ulcers on the lower extremities (see Fig. 11-13). The tumors are usually low-grade malignancies but can metastasize to regional lymph nodes and cause death. Secondary amyloidosis with hepatic and renal abnormalities.
DIFFERENTIAL DIAGNOSIS
Hypopigmented lesions with granulomas. Sarcoidosis, leishmaniasis, NTM infection, lymphoma, syphilis, and granuloma annulare.
LABORATORY EXAMINATIONS
SLIT-SKIN SMEARS A small skin incision is made; the site is then scraped to obtain tissue fluid from which a smear is made and examined after Ziehl–Neelsen staining. Specimens are usually obtained from multiple sites (both earlobes, elbows, knees, and active lesions). High Bacterial Index (BI) is seen in LL, low/negative BI can be seen in paucibacillary cases, treated cases, and cases examined by an inexperienced technician. CULTURE M. leprae has not been cultured in vitro; however, it does grow when inoculated into the mouse foot pad. Routine bacterial cultures to rule out secondary infection. PCR M. leprae DNA detected by this technique makes the diagnosis of early paucibacillary leprosy and identifies M. leprae after therapy. SEROLOGY Measure IgM antibodies to phenolic glycolipid-1 (PGL-1). DERMATOPATHOLOGY TL shows epithelioid cell granulomas forming around dermal nerves; AFB are sparse or absent. LL shows an extensive cellular infiltrate separated from the epidermis by a narrow zone of normal collagen. Skin appendages are destroyed. Macrophages are filled with M. leprae, having abundant foamy or vacuolated cytoplasm (lepra cells or Virchow cells).
DIAGNOSIS
Made if one or more of the cardinal findings are detected: Patient from endemic area, skin lesions characteristic of leprosy with
diminished or loss of sensation, enlarged peripheral nerves, finding of M. leprae in skin or, less commonly, other sites.
COURSE
After the first few years of drug therapy, the most difficult problem is management of the changes secondary to neurologic deficits; contractures and trophic changes in the hands and feet. Uncommonly, secondary amyloidosis with renal failure can complicate long-standing leprosy. Lepra type 1 reactions last 2 to 4 months in individuals with BT and up to 9 months in those with BL. Lepra type 2 reactions (ENL) occur in 50% of individuals with LL and 25% of those with BL within the first 2 years of treatment. ENL may be complicated by uveitis, dactylitis, arthritis, neuritis, lymphadenitis, myositis, and orchitis. Lucio reaction occurs secondary to vasculitis with subsequent infarction.
TREATMENT
General principles of treatment:
• Tuberculoid: Dapsone plus rifampin.
• Lepromatous: Dapsone plus clofazimine plus rifampin.
• Eradicate infection with antilepromatous therapy.
• Prevent and treat reactions (prednisone or thalidomide).
• Reduce the risk of nerve damage.
• Educate patient to deal with neuropathy and anesthesia.
• Treat complications of nerve damage.
• Rehabilitate patient into society.
Management involves a broad multidisciplinary approach including orthopedic surgery, podiatry, ophthalmology, and physical therapy.

FIGURE 25-64 • Leprosy: Tuberculoid type Well-defined, hypopigmented, slightly scaling, anesthetic macules and plaques on the posterior trunk.

FIGURE 25-65 • Leprosy: Borderline-type A 36-year-old man. Well-demarcated, infiltrated, erythematous plaques on the face.
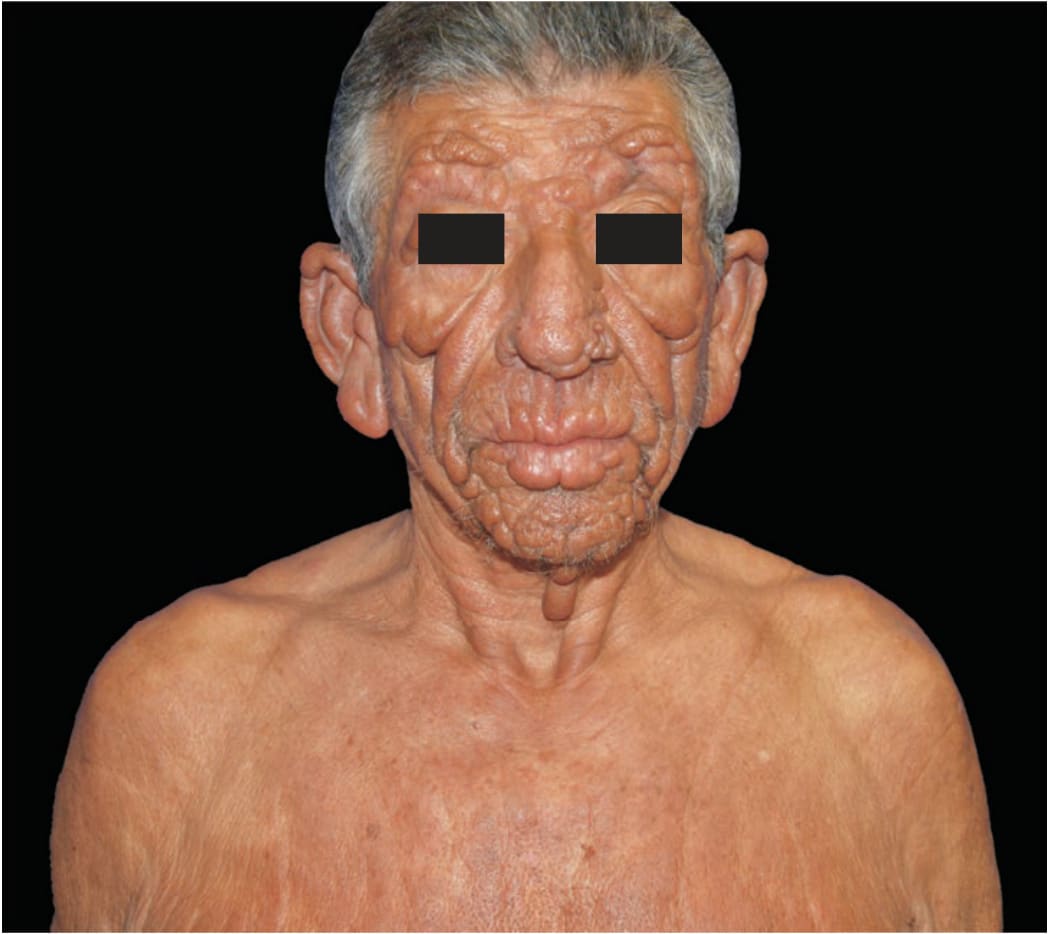
FIGURE 25-66 • Diffuse skin infiltration, multiple nodular lesions, and sensory loss are the key hallmarks of lepromatous leprosy (LL) This patient presented lesions on the upper part of the thorax, forehead, ears, nose, lips, perilabial, and mentonian regions, as well as lax skin of the malar and palpebral superior regions, with muscle force impairment on the left side. Superciliary and ciliary madarosis were also present. Ulnar and tibial posterior nerves were enlarged. A Ziehl–Neelsen stained skin smear had a 6+ bacterial index for acid-fast bacilli in clumps, and ELISA titration for anti-PGL-1 IgM was 3.445 (cutoff 0.295). The 12-month World Health Organization multidrug therapy regimen and prednisone were prescribed, with significant improvement. LL is the anergic form of leprosy; it generates an exacerbated but inefficient humoral immune response, leading to highly infectious patients. Mycosis fungoides, neurofibromatosis, sarcoidosis, amyloidosis, syphilis, anergic leishmaniasis, and lobomycosis are among diseases in the differential diagnosis. (Used with permission from Claudio G. Salgado, MD, PhD and Josafá G. Barreto, PhD, Pará Federal University, Brazil.)
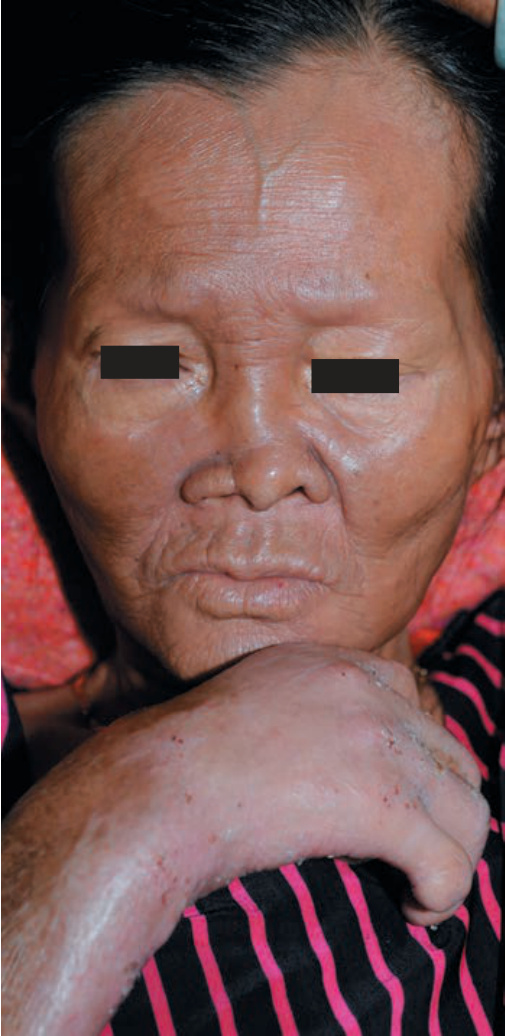
FIGURE 25-67 • Leprosy: Lepromatous type A 60-year-old Vietnamese woman with treated advanced disease. Ulnar palsy, loss of digits on right hand, and saddle-nose deformity associated with loss of nasal cartilage are seen.