LYME DISEASE
LYME DISEASE ICD-10: A69.2
• Etiologic agent: Borrelia spirochetes. Transmitted to humans by the bite of an infected Ixodes scapularis (US) or Ixodes ricinus (Europe) tick (deer tick).
• Stage 1 early localized disease: Up to 30 days post tick bite. Erythematous plaque at the tick bite site, erythema migrans (EM), noted in 70% to 80% of cases. Acute illness syndrome (fever, chills, myalgia, headache, weakness, and photophobia). Lymphocytoma.
• Stage 2 early disseminated disease: Days to weeks post tick bite. Secondary lesions. Meningitis, cranial neuritis (8%), radiculoneuritis (4%), peripheral neuritis. Carditis: AV nodal block (1%). Migratory musculoskeletal pain (33%), arthralgias.
• Stage 3 late disseminated disease: Persistent infection, developing months or years later: Intermittent or persistent arthritis, chronic encephalopathy or polyneuropathy, acrodermatitis chronica atrophicans (ACA).
• Alpha-gal syndrome: Urticaria, angioedema and/or anaphylaxis after consumption of mammalian meat or exposure to products made from mammals (e.g., milk products, gelatin, medications, cosmetics, gelatin). Tick bites from Amblyomma americanum and Ixodes ricinus species can induce IgE development to galactose-alpha-1,3- galactose (alpha-gal syndrome).
ETIOLOGY AND EPIDEMIOLOGY
ETIOLOGIC AGENT US: Borrelia burgdorferi, recently Borrelia mayonii (Midwestern US). Europe: B. afzelii, B. garinii. VECTOR Infected nymph Ixodes tick. Three stages of tick development: Larva, nymph, adult; each stage requires blood meal. Preferred host of adult Ixodes is the white-tailed deer. SEASON In the Midwestern and Eastern United States, most cases occur late May through early autumn. RISK FOR EXPOSURE Strongly associated with prevalence of tick vectors and proportion of those ticks that carry B. burgdorferi. In the northeastern United States with endemic disease, the infection rate of the nymph I. scapularis tick with B. burgdorferi is 20% to 35%. INCIDENCE LD is the most common vector-borne infection in the United States, with 25,359 cases reported in 2014. Cases reported in all 50 states except Hawaii. PATHOGENESIS After inoculation into the skin, spirochetes replicate and migrate centrifugally, producing the EM lesion, and invade vessels, spreading hematogenously to other organs. The spirochete has a particular trophism for tissues of the skin, nervous system, and joints. The organism persists in affected tissues during all stages of the illness. The immune
response to the spirochete develops gradually. Specific IgM antibodies peak between the third and sixth weeks after disease onset. The specific IgG response develops gradually over months. Proinflammatory cytokines, TNF- α, and IL-1 are produced in affected tissues.
CLINICAL MANIFESTATION
Incubation period for EM: 3 to 32 days after tick bite. Cardiac manifestations: 35 days (3 weeks to >5 months after tick bite). Neurologic manifestations: Average 38 days (2 weeks to months) after tick bite. Rheumatologic manifestations: 4 days to 2 years after bite. PRODROME With disseminated infection (stage 2), malaise, fatigue, lethargy, headache, fever, chills, stiff neck, arthralgia, myalgia, backache, anorexia, sore throat, nausea, dysesthesia, vomiting, abdominal pain, and photophobia. HISTORY Because of the small size (poppy seed) of nymph tick, most patients are unaware of tick bite; adults are sesame seed size. Bites are asymptomatic. Removal of the nymphal tick within 36 hours of attachment may preclude transmission. EM may be associated with burning sensation, itching, or pain. Only 75% of patients with Lyme disease exhibit EM. Joint complaints more common in North America. Neurologic involvement more common in Europe. With persistent disease, chronic fatigue.
STAGE 1 LOCALIZED INFECTION EM. Initial erythematous macule or papule expanding centrifugally within days to form a lesion with a distinct red border at the bite site
A
B
(Fig. 25-81). Maximum median diameter is 15 cm. As EM expands, site may remain uniformly erythematous, or several rings of varying shades of red with concentric rings
(targetoid or bull’s eye lesions). When occurring on the scalp, only a linear streak may be evident on the face or neck (Fig. 25-82). Multiple EM lesions are seen with multiple bite sites. Most common sites: Thigh, groin, and axilla. Center may become indurated, vesicular, ecchymotic, or necrotic. As EM evolves, postinflammatory hyperpigmentation, transient alopecia, and desquamation may occur. Borrelial Lymphocytoma (BL). Mainly seen in Europe. Usually arises at the site of tick bite. Some patients have a history of EM; others may show concomitant EM located around or near the lymphocytoma. Usually presents as a solitary bluish-red nodule (Fig. 25-83). Sites of predilection: Earlobe (children), nipple/ areola (adults), areola, scrotum; 3 to 5 cm in diameter. Other Cutaneous Findings. Malar rash, diffuse urticaria, and subcutaneous nodules (panniculitis). STAGE 2 DISSEMINATED INFECTION Secondary Lesions. Secondary lesions resemble EM but are smaller, migrate less, and lack central induration and may be scaly. Lesions occur at any site except the palms and soles. A few or dozens of lesions may occur; can become confluent. STAGE 3 PERSISTENT INFECTION Acrodermatitis chronica atrophicans (ACA) associated with B. afzelii infection in Europe and Asia. More common in elderly women. Initially, diffuse or localized violaceous erythema, usually on one extremity, accompanied by mild to prominent edema. Extends centrifugally over several months to years, leaving central areas of atrophy, veins, and subcutaneous tissue become prominent (Fig. 25-84). Localized fibromas and plaques are seen as subcutaneous nodules around the knees and elbows.
DIFFERENTIAL DIAGNOSIS
ERYTHEMA MIGRANS Insect bite (annular erythema caused by ticks, mosquitoes, or hymenoptera), epidermal dermatophytoses, allergic
contact dermatitis, herald patch of pityriasis rosea, and fixed drug eruption. Lyme disease-like illness with exposure in Midwest and southern United States
transmitted by Lone Star tick (Amblyomma americanum); referred to as southern tick- associated rash illness. SECONDARY LESIONS Secondary syphilis, pityriasis rosea, erythema multiforme, and urticaria.
LABORATORY EXAMINATIONS
Skin Biopsy of EM. Deep and superficial perivascular and interstitial infiltrate containing lymphocytes and plasma cells with some degree of vascular damage (mild vasculitis or hypervascular occlusion). Spirochetes can be demonstrated in up to 40% of EM biopsy specimens.
DIAGNOSIS
The CDC recommends a two-step approach: http://www.cdc.gov/lyme/. Diagnosis of early LB made on characteristic clinical findings in a person living in or having visited an endemic area; does not require laboratory confirmation. Diagnosis of late LB confirmed by specific serologic tests.
COURSE
After adequate treatment, early lesions resolve within 2 weeks and late manifestations are prevented. Late manifestations identified early usually clear after adequate antibiotic therapy. However, delay in diagnosis may result in permanent joint or neurologic disabilities. EM (short duration of infection) treated with antimicrobial agents does not confer protective immunity. If LB goes untreated for months, immunity may develop that protects against reinfection for years.
TREATMENT
Doxycycline 100 mg twice daily for 14 to 21 days is the treatment of choice for early localized and disseminated disease. Late stage Lyme disease should be treated for 14 to 28 days. Amoxicillin, cefuroxime, ceftriaxone, cefotaxime, and penicillin can be used in children under 8, pregnant woman, and doxycycline-allergic patients. A prophylactic dose of doxycycline 200 mg can be given for high risk bites within 72 hours.
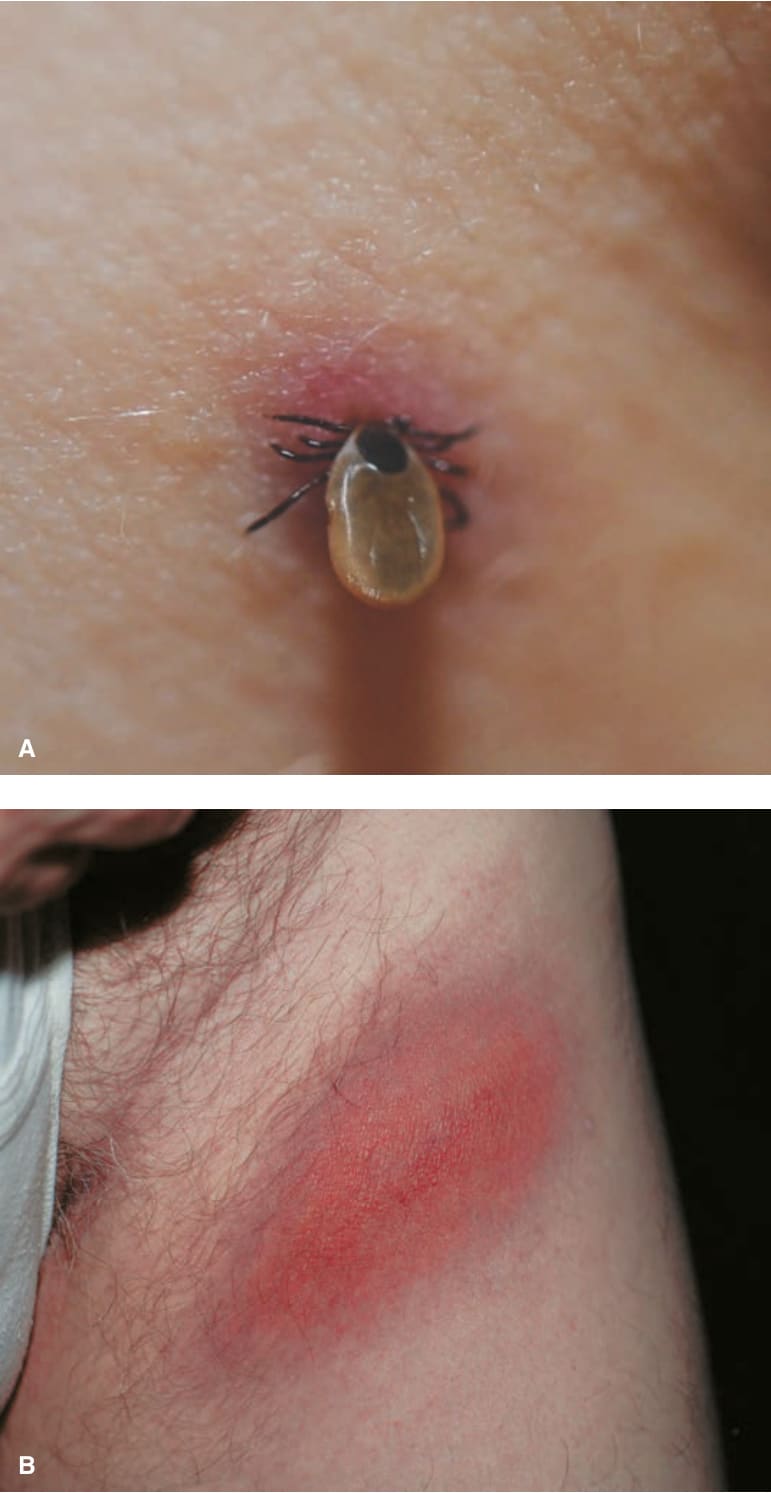
FIGURE 25-81 • Lyme borreliosis: Erythema migrans (EM) on upper thigh (A). Attachment of Ixodes tick; (B) Oval erythema, slowly increasing (i.e., migrans). Will later resolve in the center, forming a ring.

FIGURE 25-82 • Lyme borreliosis: Erythema migrans on face Serpiginous erythematous lesion on the forehead represents the margin of a large lesion occurring on the scalp.
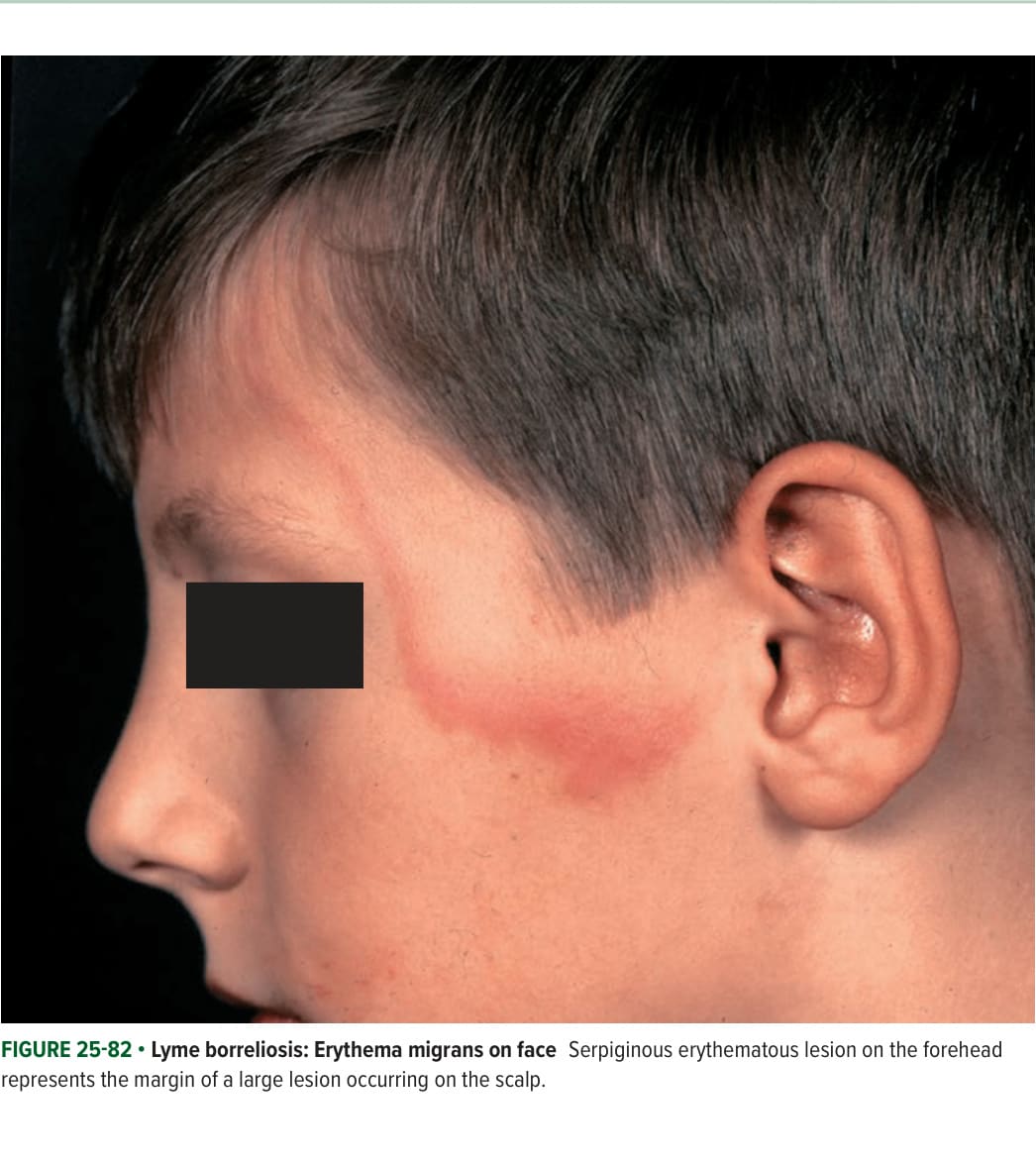
FIGURE 25-83 • Lyme borreliosis: Lymphocytoma cutis Solitary, red-purple nodule on the ear.
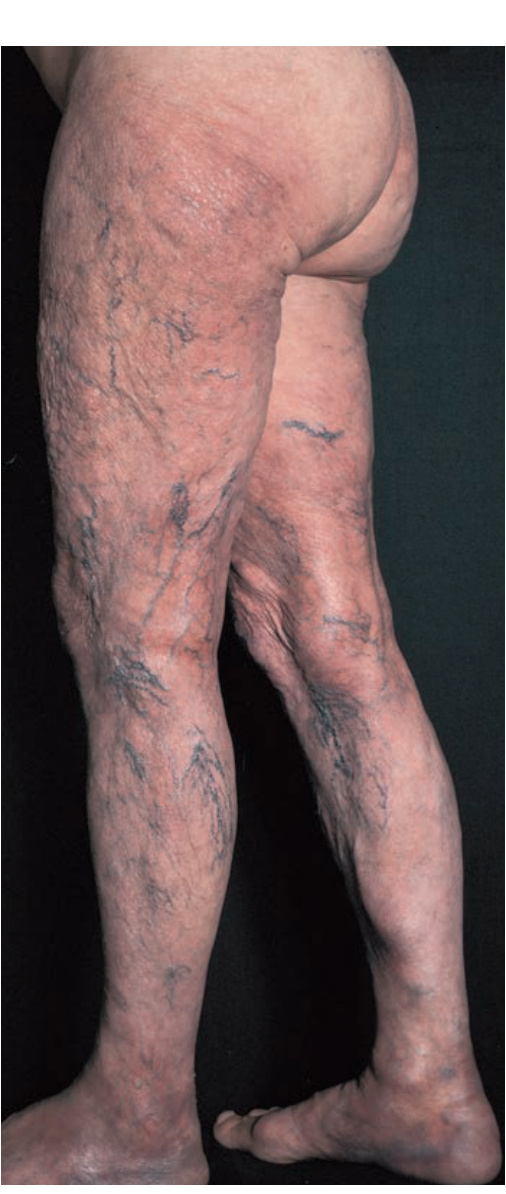
FIGURE 25-84 • Lyme borreliosis: Acrodermatitis chronica atrophicans: End stage Advanced atrophy of the epidermis and dermis with associated violaceous erythema of legs and feet; the visibility of the superficial veins is striking.