MEASLES
MEASLES ICD-10: B05
• One of the most contagious airborne diseases, it is characterized by fever, coryza, and cough; an exanthema; conjunctivitis; pathognomonic enanthem (Koplik spots).
• Significant morbidity and mortality occur in acute and chronic course.
• Childhood immunization is highly effective at preventing infection.
• Synonyms: Morbilli and rubeola.
ETIOLOGY AND EPIDEMIOLOGY
ETIOLOGY Measles virus, member of RNA genus Morbillivirus, and family Paramyxoviridae. DEMOGRAPHY Measles is no longer endemic in industrialized countries; until recently cases were primarily from importation of measles. In the last decade measles has made a resurgence in developed nations due to parents choosing not to have their children vaccinated. RISK FACTORS Unvaccinated children are at the highest risk. Transmission spread by respiratory droplets produced by sneezing and coughing. Infected persons contagious from several days before onset of rash up to 5 days after lesions appear. Ninety percent of susceptible contacts will be infected. PATHOGENESIS Virus enters cells of respiratory tract, replicates locally, spreads to regional lymph nodes, and disseminates hematogenously to skin and mucous membranes, where it replicates. Modified measles, a milder form of the illness, may occur in individuals with preexisting partial immunity induced by active or passive immunization. Persons deficient in cellular immunity are at high risk for severe measles.
CLINICAL MANIFESTATION
INCUBATION PERIOD Ten to 15 days. PRODROME Fever. Malaise. Upper respiratory symptoms (coryza, hacking bark-like cough). Photophobia, conjunctivitis with lacrimation. Periorbital edema. As exanthem progresses, systemic symptoms subside. EXANTHEM On the fourth febrile day, erythematous macules and papules appear on the forehead at hairline and behind the ears; it spreads centrifugally and inferiorly to involve the face, trunk (Fig. 27-23), extremities, and palms/soles, reaching the feet by third day. Initial discrete
lesions may become confluent, especially on the face, neck, and shoulders. Lesions gradually fade in order of appearance, with subsequent residual yellow-tan stain or faint desquamation. Exanthem resolves in 4 to 6 days. ENANTHEM Cluster of tiny bluish-white spots on red background, appearing on or after second day of febrile illness, are seen on buccal mucosa opposite premolar teeth, i.e., Koplik spots that are pathognomonic of measles. Appear before exanthem. Also: Entire buccal/ inner labial mucosa may be inflamed. BULBAR CONJUNCTIVAE Conjunctivitis, injected, and red. GENERAL EXAMINATION Generalized lymphadenopathy. Diarrhea and vomiting. Splenomegaly. MODIFIED MEASLES Milder clinical findings with preexisting partial immunity. ATYPICAL MEASLES Occurs in individuals immunized with formalin-inactivated measles vaccine, subsequently exposed to measles virus. Exanthem begins peripherally and moves centrally; can be urticarial, maculopapular, hemorrhagic, and/or vesicular. Systemic symptoms can be severe. MEASLES IN HOST WITH DEFENSE DEFECTS Rash may not occur. Pneumonitis and encephalitis more common.
DIFFERENTIAL DIAGNOSIS
DISSEMINATED MACULOPAPULAR ERUPTION Morbilliform drug eruption, scarlet fever. Kawasaki syndrome.
DIAGNOSIS
Clinical diagnosis confirmed by serology. Multinucleated giant cells in secretions. Isolate virus from blood, urine, and pharyngeal secretions. Detect measles antigen in respiratory secretions by immunofluorescent staining. Detects genomic sequences of measles virus RNA in serum, throat swabs, and cerebrospinal fluid (CSF).
A
B
C
D
COURSE
Self-limited infection in most patients, though there were 140,000+ deaths globally in 2018. Children <5 years old are at the highest risk for death. Sites of complications: respiratory tract, central nervous system (CNS). Complications more common in malnourished children, the unimmunized, and those with congenital immunodeficiency
and leukemia. Acute complications (10% of cases): otitis media, pneumonia (bacterial or measles), diarrhea, measles encephalitis, and thrombocytopenia. Chronic complication: subacute sclerosing panencephalitis (Dawson encephalitis).
TREATMENT
Prophylactic immunization. Supportive care.
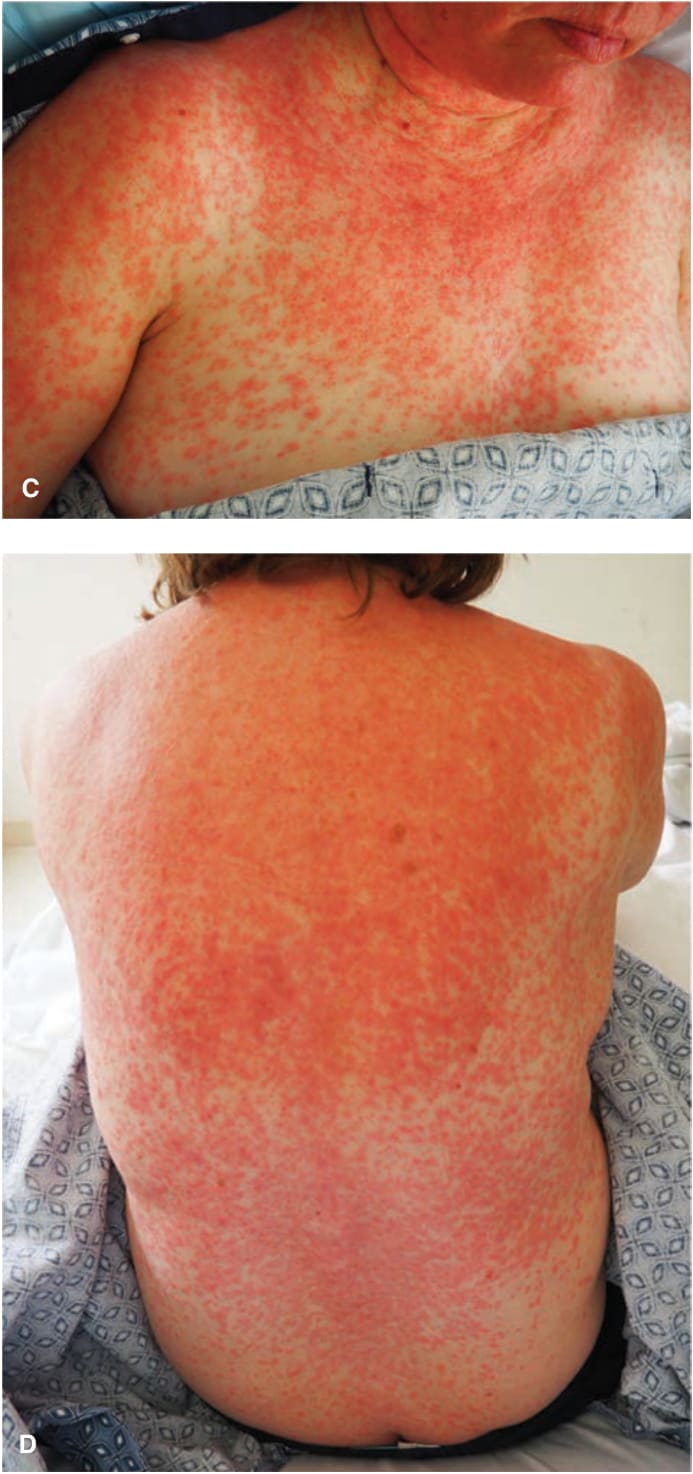
FIGURE 27-23 • Measles with exanthem (A) Erythematous macules, first appearing on the face and neck where they become confluent, spreading to the trunk and arms in 2 to 3 days where they remain discrete. In contrast, rubella also first appears initially on the face but spreads to the trunk in one day. Koplik spots on the buccal mucosa were also present. Erythematous papules have become confluent on the face on the fourth day. Measles with Koplik spots (B) Red papules on buccal mucosa opposite premolars prior of appearance of exanthema. (From the Centers for Disease Control and Prevention.) (continued)