DENGUE
DENGUE ICD10: A90
• Self-limited systemic viral infection transmitted from mosquitoes to humans.
• Incidence. Globally, 390 million infections annually, of which 96 million present with clinical symptoms.
CLINICAL SYNDROMES
DENGUE FEVER Arthralgia–rash syndrome with abrupt onset of fever and muscle and joint pains, usually with retro-orbital pain, photophobia, and lymphadenopathy. Rash: Early flushing; later macules/papules; purpura. DENGUE HEMORRHAGIC FEVER Increased vascular permeability and plasma leakage from blood vessels into tissues, thrombocytopenia, and bleeding manifestations (frank hemorrhage to spontaneous petechiae or elicited by tourniquet test). Plasma leakage causes a rise in hematocrit, effusions, and edema, especially in the chest and abdomen (Fig. 27-29). DENGUE SHOCK SYNDROME Occurs when leakage or bleeding, or both, are sufficient to induce hypovolemic shock.
ETIOLOGY AND EPIDEMIOLOGY
ETIOLOGY Flavivirus, single-stranded RNA virus. Four distinct dengue serotypes (DEN-1, 2, 3, 4). Arthropod-borne virus (arbovirus). Infection confers lifelong protection against that serotype, but cross-protection between serotypes is of
short duration. Infection with virus of a different serotype after the primary attack is more apt to result in severe disease, dengue hemorrhagic fever, or dengue shock syndrome. VECTOR Transmitted by the bite of the A. aegypti mosquito; less commonly A. albopictus. Mosquito acquires virus by feeding upon viremic human; remains infective for life. DEMOGRAPHY 2.5 billion people live in dengue endemic areas; 50 to 100 million cases of dengue occur annually worldwide. Most cases occurring in United States are imported in travelers returning from the tropics. Yearround transmission between latitudes 25°N and 25°S. Increased incidence associated with rapid urban population growth, overcrowding, lax mosquito control, and climate change. PATHOGENESIS Pre-existing dengue antibodies are associated with more severe disease. Virus–antibody complexes formed within a few days of second dengue infection; nonneutralizing enhancing antibodies promote infection of higher numbers of mononuclear cells, followed by release of cytokines, vasoactive mediators, and procoagulants, leading to the disseminated intravascular coagulation.
A B
CLINICAL MANIFESTATION
INCUBATION PERIOD Three to 7 days after bite of infected mosquito. Most dengue virus infections are asymptomatic. FEBRILE PHASE High temperature (≥38.5°C) accompanied by headache, vomiting, myalgia, and joint pain. In some cases, a transient macular rash (Fig. 27-29A). Petechiae and bruising may be noted at venipuncture sites (Fig. 27-29B). Lasts for 3 to 7 days after which most patients recover with complications. CRITICAL PHASE Becomes apparent around the time of defervescence, evidenced by increasing hemoconcentration, hypoproteinemia, pleural effusions, and ascites. Hemorrhagic manifestations occur, manifested by major skin bleeding, gastrointestinal (GI), or vaginal bleeding. Moderate-to-severe thrombocytopenia common, followed by rapid recovery during recovery phase. RECOVERY PHASE Altered vascular permeability resolves after 48 to 72 hours. A second
rash may be appearing during recovery phase, mild macules/papules to severe, pruritic suggesting leukocytoclastic vasculitis. Rash resolves with desquamation over 1 to 2 weeks. Profound fatigue persists for several weeks after recovery.
DIFFERENTIAL DIAGNOSIS
Other arboviral infection such as chikungunya and viral exanthems. Disease with local prevalence: Typhoid, malaria, leptospirosis, viral hepatitis, rickettsial diseases, and bacterial sepsis.
DIAGNOSIS
Consider diagnosis in travelers with febrile illness recently returned from endemic areas. During febrile phase, detection of viral nucleic acid in serum diagnostic. IgM seroconversion between paired samples is confirmatory finding.
TREATMENT
Symptomatic supportive therapy (http://www. cdc.gov/dengue/).
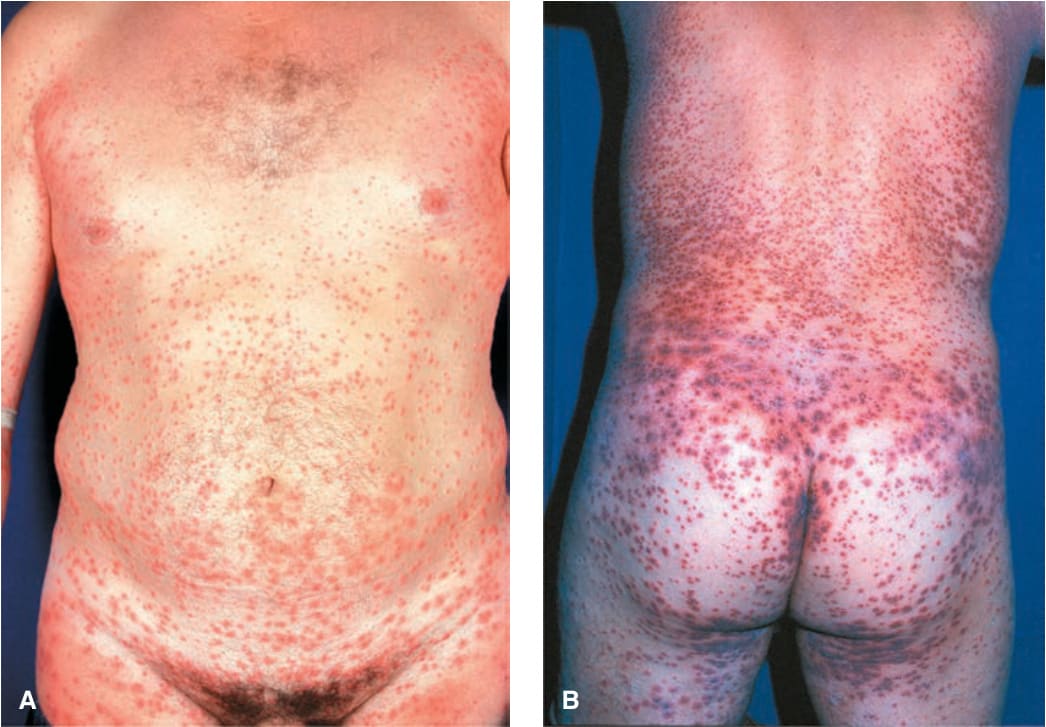
FIGURE 27-29 • Dengue hemorrhagic fever A 39-year-old with fever and rash after a trip to Malaysia. Dermal hemorrhage and petechiae on normal tanned (A) and white skin are seen on the buttocks 48 hours later (white islands in a sea of red [B]). (Reproduced with permission from Hafner C et al. Hemorrhagic dengue fever after trip to Malaysia. Hautarzt. 2006;57(8):705–707. © Springer 2005.)