SCABIES
SCABIES ICD-10: B86
• Superficial epidermal infestation by the mite Sarcoptes scabiei var. hominis. Transmission: Usually spread by skin-to-skin contact and fomites.
• Clinical Manifestation. Pruritus often with minimal cutaneous findings. Burrows under stratum corneum.
• Scabetic Nodules. Eczematous dermatitis. Hyperinfestation (crusted or hyperkeratotic or Norwegian scabies).
• Diagnosis. Easily missed and should be considered in a patient of any age with persistent generalized severe pruritus.
ETIOLOGY AND EPIDEMIOLOGY
ETIOLOGIC AGENT S. scabiei var. hominis. Obligate human parasite. Mites of all developmental stages burrow into epidermis shortly after contact, no deeper than stratum granulosum; deposit feces in tunnels (Fig. 28-16). Female life span 4 to 6 weeks; lays 40 to 50 eggs at the rate of 3 eggs per day in skin. These eggs hatch in 4 days, at which time they migrate to the skin surface and mature into adults. After mating, the pregnant female re-enters the epidermis to repeat the life cycle. An infected person typically carries ~12 living mites., though there can be up 2 million mites in cases of Norwegian scabies. DEMOGRAPHY Major public health problem in many resource-poor countries, especially in areas with a hot, tropical climate and high density. In some of these areas, it is thought
that infection prevalence is 5–10% in children. The World Health Organization estimates that there are ~130 million cases/year globally. In countries where human T-cell leukemia/ lymphoma virus (HTLV-I) disease is common, scabies hyperinfestation can a marker of this disease. Transmission by skin-to-skin contact and fomites. Mites can remain alive for >2 days on clothing or in bedding. Persons with hyperinfestation shed many mites into their environment daily and pose a high risk of infecting those around them.
PATHOGENESIS
Hypersensitivity of both immediate and delayed types occurs in the development of lesions other than burrows. During first infestation, pruritus occurs after sensitization to S. scabiei has occurred, usually within 4 to
6 weeks. After reinfestation, pruritus may occur within 24 hours. With hyperinfestation, persons are often immunocompromised or have neurologic disorders.
CLINICAL MANIFESTATION Symptoms Patients are often aware of similar symptoms in family members or sexual partners. Pruritus is intense, widespread, but usually spares the head and neck. Itching often interferes with or prevents sleep. Pruritus may be absent with hyperinfestation. Rash ranges from no rash to generalized erythroderma. Patients with atopic diathesis scratch, producing eczematous dermatitis. Some individuals experience pruritus for many months with no rash. Tenderness of lesions suggests secondary bacterial infection.
Cutaneous Findings (1) Lesions occurring at the sites of mite infestation, (2) cutaneous manifestations of hypersensitivity to mites, (3) lesions secondary to chronic rubbing and scratching, (4) secondary infection, (5) hyperinfestation, and (6) variants of scabies in special hosts: those with an atopic diathesis, nodular scabies, scabies in infants/small children, and scabies in the elderly. INTRAEPIDERMAL BURROWS Skin-colored ridges, 0.5 to 1 cm in length (Figs. 28-17 to 28-19), either linear or serpiginous, with minute vesicle or papule at end of tunnel. Each infesting woman mite produces one burrow. Mites are about 0.5 mm in length. Burrows average 5 mm in length but may be up to 10 cm. Distribution: Areas with few or no hair follicles, usually where stratum corneum is thin and soft, i.e., the interdigital webs of the hands (Fig. 28-17), wrists, palms, and soles in infants (Fig. 28-18), shaft of penis, elbows, feet, buttocks, or axillae (Figs. 28-19 and 28-20). In infants, infestation may also occur on head and neck. Scabies with nodules 5 to 20 mm in diameter, red, pink, tan, or brown in color, smooth (Fig. 28-21); burrow sometimes seen on the surface of a very early lesion. Distribution: Scrotum, penis (Fig. 28-21), axillae, waist, buttocks (Fig. 28-22), or areolae. Resolve with
postinflammatory hyperpigmentation. May be more apparent after treatment, as eczematous eruption resolves. SCABIES WITH HYPERINFESTATION (FORMERLY CALLED NORWEGIAN SCABIES) May begin as ordinary scabies. In others, clinical appearance is of chronic eczema, psoriasiform dermatitis, seborrheic dermatitis, or erythroderma. Lesions often markedly hyperkeratotic and/ or crusted (Figs. 28-23 and 28-24). Warty dermatosis of the hands/feet with nail bed hyperkeratosis (Fig. 28-24B). Erythematous scaling eruptions occur on the face, neck, scalp, and trunk. Affected persons have a characteristic odor. Distribution: Generalized (even involving head and neck in adults) or localized. In patients with neurologic deficit, hyperinfestation may occur only in an affected limb. May be localized only to the scalp, face, finger, toenail bed, or sole. “Id” or autosensitization-type reactions characterized by widespread small urticarial edematous papules mainly on the anterior trunk, thighs, buttocks, and forearms. SECONDARY CHANGES Excoriations, lichen simplex chronicus, and prurigo nodules. Postinflammatory hyper- and hypopigmentation in more deeply pigmented individuals. Bullous scabies can mimic bullous pemphigoid. Secondary infection by S. aureus.
DIFFERENTIAL DIAGNOSIS
Pruritus, localized or generalized, rash delusions of parasitosis, adverse cutaneous drug reaction, atopic dermatitis, allergic contact dermatitis, and metabolic pruritus. Nodular scabies. urticaria pigmentosa (in young child), papular urticaria (insect bites), prurigo nodularis, and pseudolymphoma. SCABETIC HYPERINFESTATION Psoriasis, eczematous dermatitis, seborrheic dermatitis, and erythroderma.
LABORATORY EXAMINATIONS
MICROSCOPY Highest yield in identifying a mite is in typical burrows on the finger webs, flexor aspects of wrists, and penis. A drop of mineral oil is placed over a burrow, and the burrow is scraped off with a curette or no. 15 scalpel blade and placed on a microscope slide. Three findings are diagnostic of scabies:
A
B
A
B
A
B
Burrows
Common sites
Common sites
Burrows
A
C
B
D
A
B
S. scabiei mites, eggs, and fecal pellets (scybala) (Fig. 28-24). DERMATOPATHOLOGY Scabietic burrow: Located within stratum corneum; woman mite with eggs situated in blind end of burrow. Spongiosis (epidermal edema) near mite with vesicle formation is common. Dermis shows infiltrate with eosinophils. Nodules: Dense chronic inflammatory infiltrate with eosinophils. In some cases, persistent arthropod reaction resembling lymphoma with atypical mononuclear cells. Hyperinfestation: Thickened stratum corneum riddled with innumerable mites.
DIAGNOSIS
Clinical findings, confirmed by microscopy (identification of mites, eggs, or mite feces).
COURSE
Pruritus often persists up to several weeks after successful eradication of mite infestation, understandable in that the pruritus is a hypersensitivity phenomenon to mite antigen(s). If reinfestation occurs, pruritus becomes symptomatic within a few days. Delusions of parasitosis can occur in individuals who have been successfully treated for scabies or have never had scabies. Hyperinfestation: May be impossible to eradicate; recurrence more likely to relapse than reinfestation. Nodules: In treated patients, 80% resolve in 3 months but may persist up to 1 year.
MANAGEMENT
PRINCIPLES OF TREATMENT Treat infested individuals and close physical contacts (including sexual partners) at the same time, whether or not symptoms are present. Application should be to all skin sites. RECOMMENDED REGIMENS Permethrin 5%. Cream applied to all areas of the body.
Lindane (g-Benzene Hexachloride) 1% lotion or cream applied thinly to all areas of the body from the neck down; wash off thoroughly after 8 hours. Note: Lindane should not be used after a bath or shower, or by patients with extensive dermatitis, pregnant or lactating women, or children younger than 2 years. Mite resistance to lindane exists. Low cost makes lindane a key alternative in many countries. ALTERNATIVE REGIMENS Topical. Crotamiton 10%, sulfur 2% to 10% in petrolatum, benzyl benzoate 10% and 25%, benzyl benzoate with sulfiram, malathion 0.5%, sulfram 25%, and ivermectin 0.8%. Systemic. Oral ivermectin, 200 µg/kg; single dose reported very effective in 15 to 30 days. Two to three doses, separated by 1 to 2 weeks, usually required for heavy infestation or in immunocompromised individuals. May effectively eradicate epidemic or endemic scabies in institutions such as nursing homes, hospitals, and refugee camps. Not approved by U.S. Food and Drug Administration. Do not use in infants, young children, or pregnant/ lactating women. CRUSTED SCABIES Oral ivermectin combined with topical scalicides (not ivermectin). Decontamination of the environment. NODULES of scabies resolve after intralesional injection of triamcinolone acetonide. POSTSCABIETIC ITCHING Generalized itching that persists a week or more is probably caused by hypersensitivity to remaining dead mites and mite products. Antihistamines, topical steroids can be used. For severe, persistent pruritus, especially in individuals with a history of atopic disorders, a 14-day tapered course of prednisone is indicated. SECONDARY BACTERIAL INFECTION Treat with mupirocin ointment or systemic antimicrobial agent.
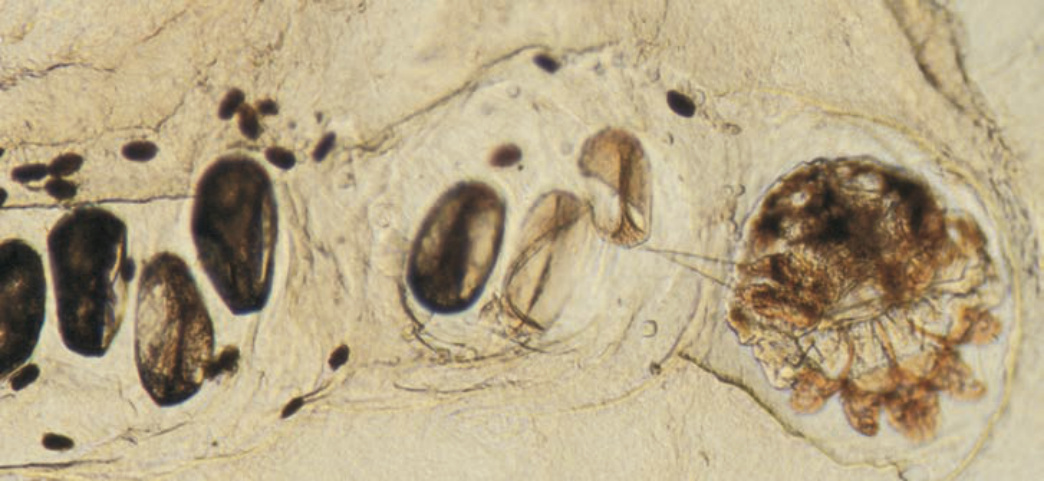
FIGURE 28-16 • Burrow with Sarcoptes scabiei (female), eggs, and feces Female mite at the end of a burrow with seven eggs and smaller fecal particles obtained from a papule on the webspace of the hand.
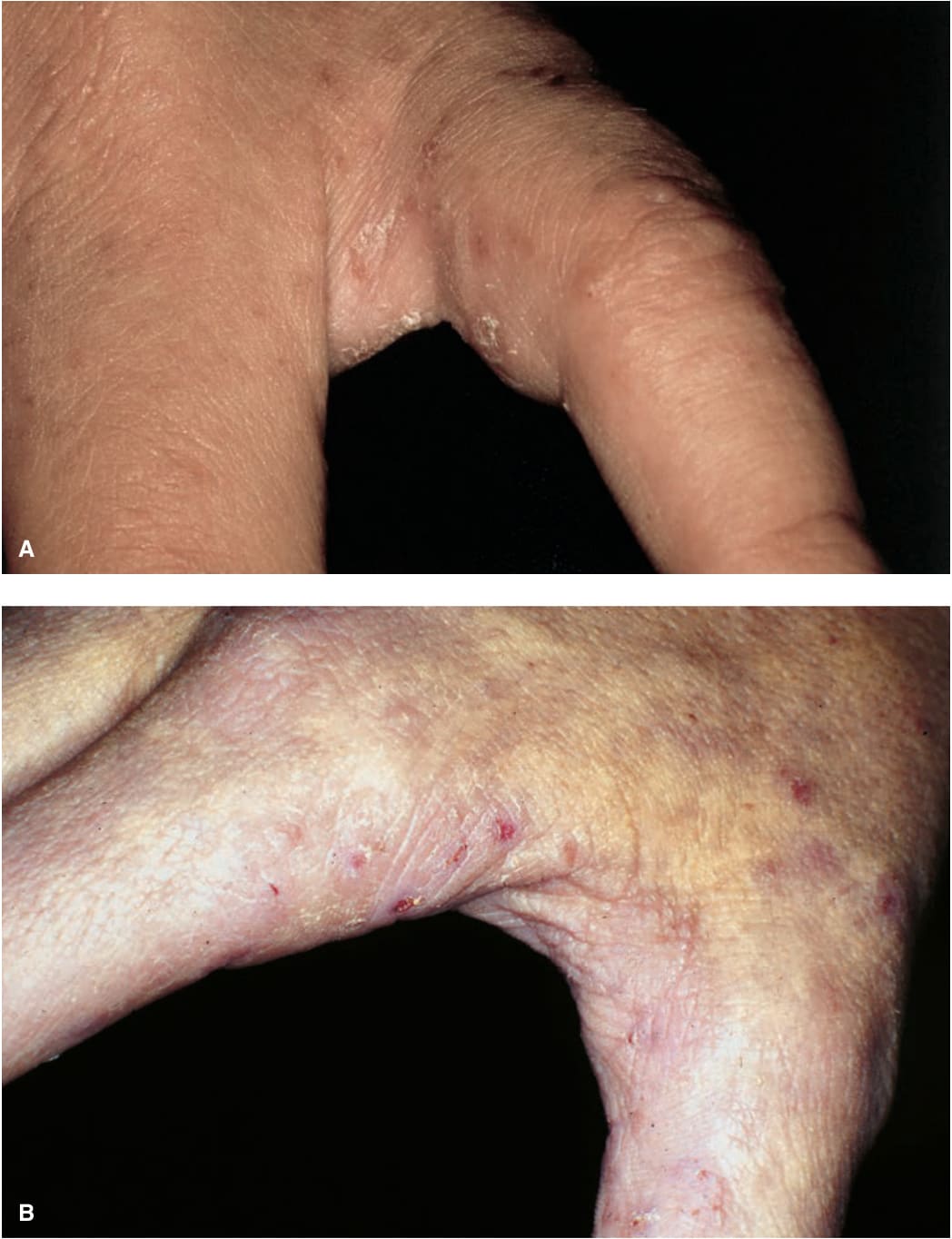
FIGURE 28-17 • (A, B) Scabies with burrows Papules and burrows in typical location on the finger webs. Burrows are tan or skin-colored ridges with linear configuration with a minute vesicle or papule at the end of the burrow; they are often difficult to define.

FIGURE 28-18 • (A, B) Burrows of scabies on the palm and wrist of a 3-year-old boy. There are many linear and even semi-circular lesions. The whole family was affected.

FIGURE 28-19 • (A,B) Burrows on penis shaft, scrotum, and groin If you suspect scabies in a man, always look at the penis.
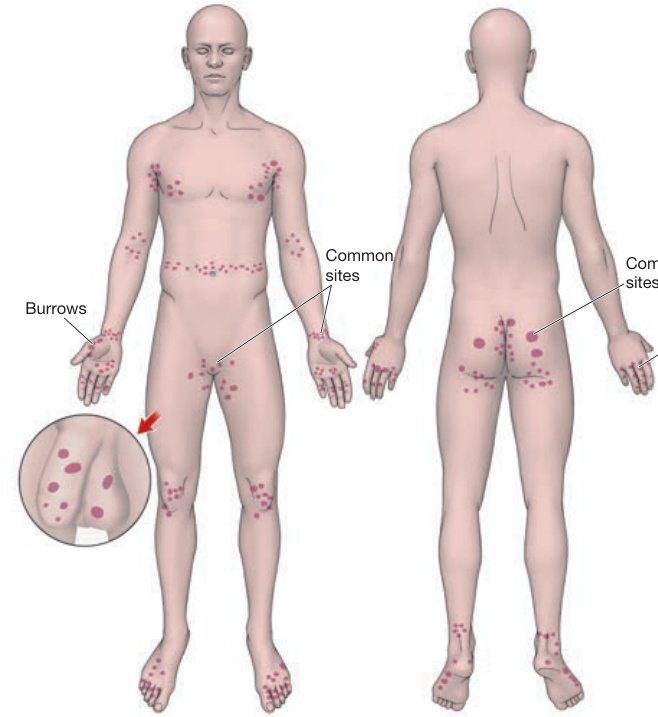
FIGURE 28-20 • Scabies: Predilection sites Burrows are most easy to identify on the webspace of the hands, wrists, and lateral aspects of the palms. Scabietic nodules occur uncommonly, arising on the genitalia, especially the penis and scrotum, waist, axillae, and areolae.

FIGURE 28-21 • Scabies with nodules Red-brown papules and nodules on the penis and scrotum; these lesions are pathognomonic for scabies, occurring at sites of infestation in some individuals.

FIGURE 28-22 • Scabies with nodules A 4-month-old infant with reddish brown nodules on thigh and buttocks persisting after treatment with permethrin.

FIGURE 28-23 • (A–D) Crusted Scabies A 40-year-old woman with systemic sclerosis on immunosuppression with full body scale, redness, and crusting. Hyperkeratotic crusts of the perioral skin are pathognomonic for this variant of scabies. Pruritus was excruciating. Note the clubbing of nails and decrease oral aperture from systemic sclerosis.
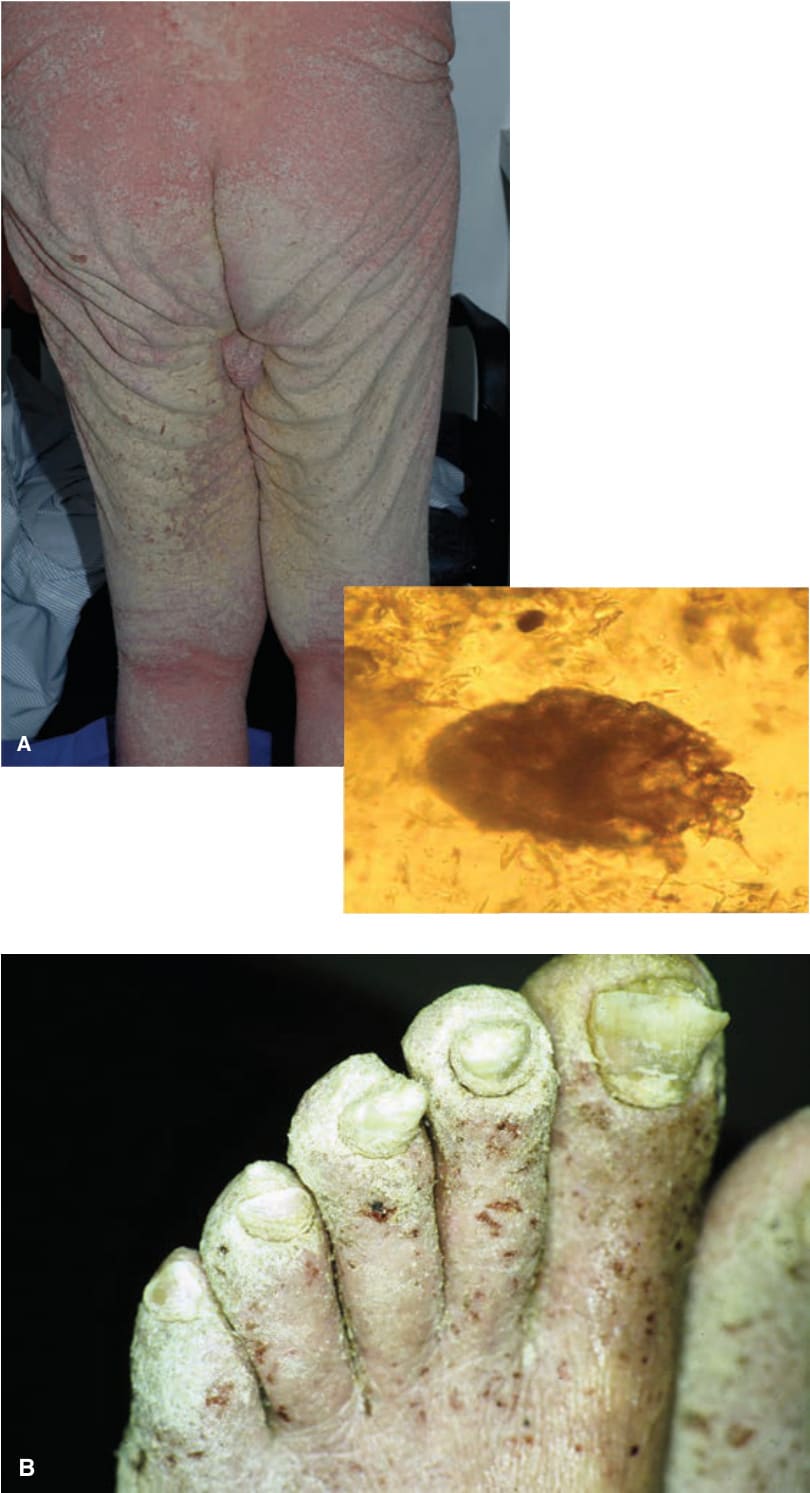
FIGURE 28-24 • Scabies with hyperinfestation (A) A 79-year-old man with hyperkeratotic scabies for 4 years. The patient had been treated in his home with topical antiscabetic agents and oral ivermectin as well as extensive decontamination of his home on multiple occasions. Confluent hyperkeratotic plaques are seen on the back, buttocks, and legs. As many as five scabetic mites were seen on one microscope field (see inset). (B) A 50-yearold man with HIV and crusted scabies leading to powdery crusting of the toes.