SECONDARY SYPHILIS
SECONDARY SYPHILIS ICD-10: A51.3
CLINICAL MANIFESTATION
Appears 2 to 6 months after primary infection; 2 to 10 weeks after appearance of the primary chancre; 6 to 8 weeks after healing of the chancre. Chancre may still be present when secondary lesions appear (15% of cases). Concomitant HIV infection may alter the course of secondary syphilis. Fever, sore throat, weight loss, malaise, anorexia, headache, and meningismus. Mucocutaneous lesions are asymptomatic.
SKIN LESIONS OF SECONDARY SYPHILIS Macules and papules 0.5 to 1 cm, round to oval; pink brownish-red. First exanthem always macular and faint (Fig. 30-27A,B). Hypopigmented and non-scaling patches around the neck is termed the necklace of Venus in secondary syphilis (Fig. 30-27B). Later eruptions may be papulosquamous (Figs. 30-28 and 30-29), pustular, or acneiform. Vesiculobullous lesions occur only in neonatal congenital syphilis (palms and soles). On the palms and soles
A
B
A B
lesions are psoriasiform (Figs. 30-30 and 30-31). On palpation, papules are firm (Figs. 30-30 and 30-31); condylomata lata, soft. In the face, they look like seborrheic dermatitis and occur on the forehead and the nasolabial folds (Fig. 30-29). Lesions may also be annular or polycyclic,
A
B
especially on the face in dark-skinned persons (Fig. 30-32). In relapsing secondary syphilis, arciform lesions. Always sharply defined except for macular exanthem. Lesions are scattered, tend to remain discrete, and are usually symmetric.
A B
Condylomata lata (Fig. 30-33). Most commonly in the anogenital region and mouth; can be seen on any body surface where moisture can accumulate between intertriginous surfaces, that is, axillae or toe webs. HAIR Diffuse hair loss, including temples and parietal scalp. Patchy, moth-eaten alopecia on the scalp and beard area. Loss of eyelashes or lateral third of eyebrows. MUCOUS MEMBRANES Small, asymptomatic, round or oval, slightly elevated, flat-topped macules and papules 0.5 to 1 cm in diameter, covered by hyperkeratotic white to gray membrane, occurring on the oral or genital mucosa. Split papules at the angles of the mouth. GENERALIZED LYMPHADENOPATHY Cervical, suboccipital, inguinal, epitrochlear, or axillary. Splenomegaly. ASSOCIATED FINDINGS Musculoskeletal involvement: Periostitis of long bones, particularly tibia (nocturnal pain); arthralgia; hydrarthrosis of knees or ankles without x-ray changes. Eyes: Acute bacterial iritis, optic neuritis, and uveitis. Meningovascular reaction: CSF positive for inflammatory markers. Gastrointestinal (GI) involvement: Diffuse pharyngitis, hypertrophic gastritis, hepatitis, patchy proctitis, ulcerative colitis, and rectosigmoid mass. Genitourinary involvement: Glomerulonephritis and nephrotic syndrome, cystitis, and prostatitis.
LABORATORY EXAMINATIONS
DERMATOPATHOLOGY Epidermal hyperkeratosis; capillary proliferation with endothelial swelling; perivascular infiltration by monocytes, plasma cells, and lymphocytes. Spirochete is present in many tissues including the skin, eye, and CSF. CSF Abnormal in 40% of patients. Spirochetes in CSF in 30% of cases. LIVER FUNCTION Elevated enzymes. RENAL FUNCTION Immune complex-induced membranous glomerulonephritis.
COURSE
Recurrent eruptions appear after month-long asymptomatic intervals. Initially a relatively
A
B
C
faint exanthem, always macular, pink; lesions are ill defined. Later lesions of early syphilis are papular, brownish, and tend to be more localized. Symptoms may last 2 to 6 weeks (4 weeks average) and may recur in untreated or inadequately treated patients. Secondary lesions subside within 2 to 6 weeks, with the infection entering the latent stage.
DIFFERENTIAL DIAGNOSIS
EXANTHEM Adverse cutaneous drug eruption, pityriasis rosea, viral exanthem, infectious
mononucleosis, tinea corporis, tinea versicolor, scabies, “id” reaction, condylomata acuminata, acute guttate psoriasis, and lichen planus.
DIAGNOSIS
Clinical suspicion confirmed by lab tests. Dark-field is positive in all secondary syphilis lesions except for macular exanthem.
TREATMENT
As for primary syphilis (see p. 809).
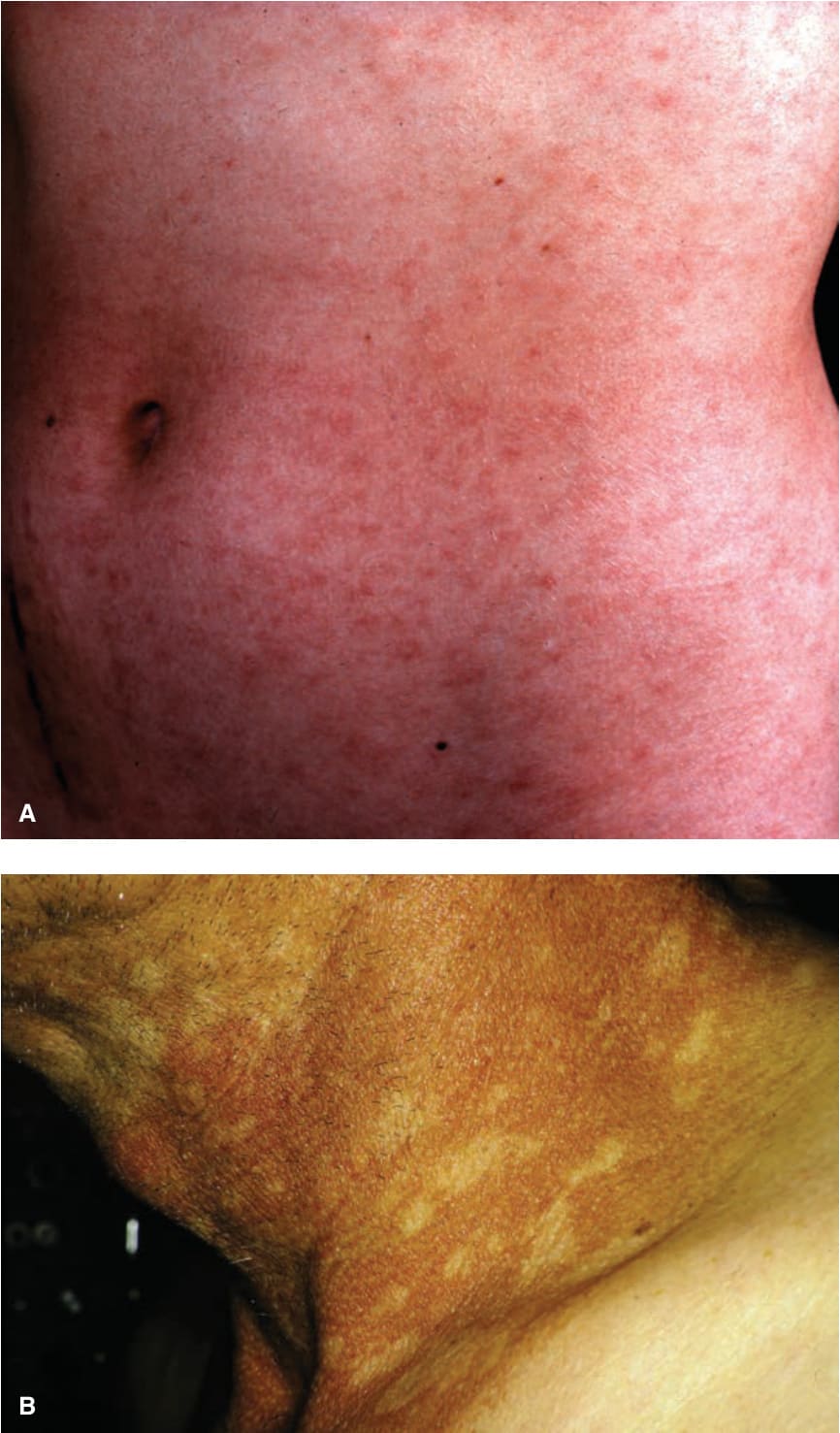
FIGURE 30-27 • Secondary syphilis (A) A 21-year-old woman with the first exanthem of secondary syphilis (roseola syphilitica). These are barely visible, relatively ill-defined macules of salmon color, disseminated over chest, abdomen, and back. Similar to pityriasis rosea but without or very little scale. (B) A 52-year-old man with hypopigmented nonscaly patches of only the neck in a background of subtle erythema. This is the necklace of Venus.

FIGURE 30-28 • (A,B) Secondary syphilis Later exanthema, papulosquamous and of more tan or copper-like color.
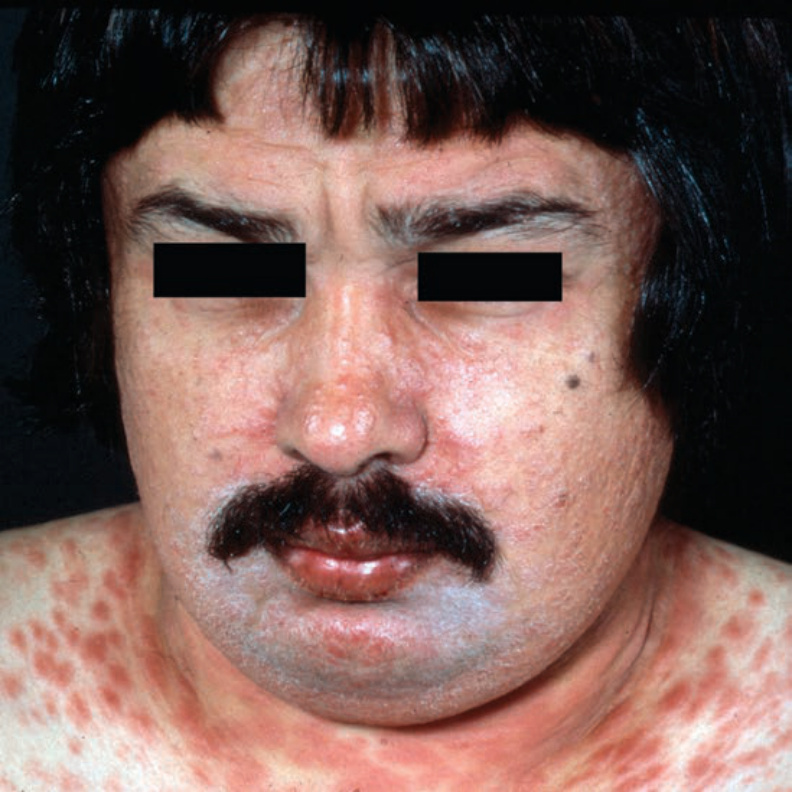
FIGURE 30-29 • Secondary syphilis Later exanthem. Seborrheic dermatitis such as papulosquamous lesions on the face and a copper tone papular rash on the neck and trunk.

FIGURE 30-30 • Secondary syphilis: papulosquamous lesion Typical red (A) and dark brown (B) keratotic papules and plaques on the palms.

FIGURE 30-31 • Secondary syphilis: papulosquamous lesions Soles of the feet with hyperpigmented (A) or dull red (B), hyperkeratotic, scaling plaques. Similar lesions are present on the palms (B).

FIGURE 30-32 • Secondary syphilis: annular facial lesions Annular plaques merging on the face of a South African woman. (Used with permission from Jeffrey S. Dover, MD.)

FIGURE 30-33 • Secondary syphilis: condylomata lata (A) Soft, flat-topped, moist, pink-tan papules and nodules on the perineum and perianal area. (B) Moist and exudative white nodules on the vulvar and perineal skin. (C) Moist pink nonexudative nodules of the vulva, perineum, and inguinal canals. The lesions are teeming with T. pallidum.