CHANCROID
CHANCROID ICD-10: A57
• Etiology: Haemophilus ducreyi, a gram-negative streptobacillus.
EPIDEMIOLOGY AND ETIOLOGY
ETIOLOGY Haemophilus ducreyi, a gram-negative streptobacillus. DEMOGRAPHY Uncommon in industrialized nations. Endemic in tropical and subtropical developing countries, especially in poor, urban, and seaport populations. Much more common in young males. Lymphadenitis more common in males. TRANSMISSION Most likely during sexual intercourse with partner who has H. ducreyi genital ulcer. Chancroid is a cofactor for HIV/ AIDS transmission; high rates of HIV/AIDS infection among those who have chancroid. Ten percent of individuals with chancroid acquired in the United States are coinfected with T. pallidum and HSV. PATHOGENESIS Primary infection develops at the site of inoculation (break in epithelium), followed by lymphadenitis. The genital ulcer is characterized by perivascular and interstitial infiltrates of macrophages and of CD4+ and CD8+ lymphocytes, consistent with a delayed-type hypersensitivity, cell-mediated immune response. CD4+ cells and macrophages in the ulcer may explain the facilitation of transmission of HIV/AIDS in patients with chancroid ulcers.
CLINICAL MANIFESTATION
Incubation period is 4 to 7 days. PRIMARY LESION Tender papule with erythematous halo that evolves to pustule, erosion, and ulcer. Ulcer is usually quite tender or painful. Its borders are sharp, undermined, and not indurated (Figs. 30-36 and 30-37). Base is friable with granulation tissue and covered with gray to yellow exudate. Edema of prepuce common. Ulcer may be singular or multiple, merging to form large or giant ulcers (>2 cm) with serpiginous shape. DISTRIBUTION Male: Prepuce, frenulum, coronal sulcus, glans penis, and shaft. Female: External genitalia, vaginal wall by direct extension from introitus, cervix, perianal.
Extragenital lesions: Breast, fingers, thighs, oral mucosa. Bacterial superinfection of ulcers can occur. Multiple ulcers (Fig. 30-37) develop by autoinoculation. PAINFUL INGUINAL LYMPHADENITIS Usually unilateral, occurs in 50% of patients 7 to 21 days after primary lesion. Ulcer may heal before buboes occur. Buboes occur with overlying erythema and may drain spontaneously. Painful ulcer at the site of inoculation, usually on the external genitalia. REGIONAL LYMPH NODES Tender adenopathy. Suppurative adenopathy. STI most strongly associated with increased risk for HIV/AIDS transmission. Synonyms. Soft chancre, ulcus molle, and chancre mou.
DIFFERENTIAL DIAGNOSIS
GENITAL ULCER GH, primary syphilis, LGV, and traumatic lesions. TENDER INGUINAL MASS GH, secondary syphilis, LGV, incarcerated hernia, plague, and tularemia.
DIAGNOSIS
Combination of a painful ulcer with tender lymphadenopathy (one-third of patients) is suggestive of chancroid. Smear: Short gram-negative rods in linear arrangement. A definitive diagnosis of chancroid requires the identification of H. ducreyi on special culture media. Rule out HIV, T. pallidum, and HSV coinfection.
COURSE
The time required for complete healing is related to the size of the ulcer; large ulcers may require 14 days. Complete resolution of fluctuant lymphadenopathy is slower than that of ulcers and may require needle aspiration through adjacent intact skin, even during successful therapy.
TREATMENT
Azithromycin 1 g in single dose. Ciprofloxacin 500 mg twice daily for 3 days (contraindicated in pregnancy). Erythromycin base 500 mg three times daily for 7 days. Intramuscular ceftriaxone in single dose. Resistance to ciprofloxacin and erythromycin has been reported.
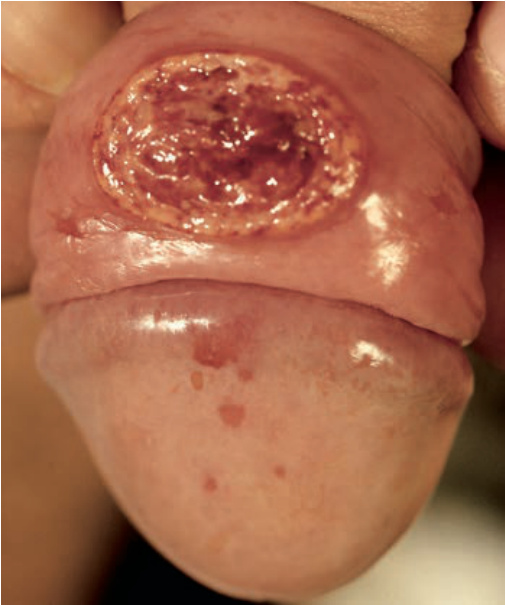
FIGURE 30-36 • Chancroid Painful ulcer with marked surrounding erythema and edema. (Used with permission from Prof. Alfred Eichmann, MD.)

FIGURE 30-37 • Chancroid Multiple, painful, punchedout ulcers with undermined borders on the vulva occurring after autoinoculation.