ONYCHOMYCOSIS
ONYCHOMYCOSIS
• Fungal infection of the nail plate.
• More common in the elderly (affects 50% of people over 70 years).
• Usually, toenails affected.
CLASSIFICATION BY ANATOMIC SITE INVOLVED
DISTAL AND LATERAL SUBUNGUAL ONYCHOMYCOSIS (DLSO) (Fig. 32-19) Most common type. Infection begins at a disrupted hyponychium,
resulting in discoloration and distal dystrophy and hyperkeratosis. When fingernails are involved, associated with skin involvement of two feet and one hand. SUPERFICIAL WHITE ONYCHOMYCOSIS (SWO) Pathogen invades surface of dorsal nail
(Fig. 32-20). Etiology: Trichophyton mentagrophytes or T. rubrum (children). Much less commonly, mold: Acremonium, Fusarium, and Aspergillus terreus. PROXIMAL SUBUNGUAL ONYCHOMYCOSIS (PSO) Pathogen enters by way of the proximal nail fold, and affects the ventral side of the proximal nail plate (Fig. 32-21). Etiology: T. rubrum. Associated with immunocompromised states.
ENDONYX
Fungal infection of the interior nail plate, sparing the nail bed. Presents with white discoloration. T. soudanense is the most
common cause, though T. rubrum can also be responsible.
ETIOLOGY AND EPIDEMIOLOGY
AGE OF ONSET More common in adults. Once acquired, usually does not remit
Debridement Debride dystrophic nails with urea cream or sterile nail clippers.
Topical agents Available as lotions and lacquer. Usually not effective except for SWO.
Systemic agents Daily dosing: 6 weeks for fingernails, 12 weeks for toenails Pulse dosing: 2–3 months for fingernails, 3–4 months for toenails Note: In systemic treatment of onychomycosis, nails usually do not appear normal after the treatment times recommended because of slow growth of nail.
Terbinafine (Allylamine) Daily dose: 250 mg Pulse dose: 500 mg daily × 1 week/month Most effective for dermatophytes
Itraconazole Daily dose: 200 mg Pulse dose: 400 mg daily × 1 week/month Effective for dermatophytes and Candida
Fluconazole: Pulse dose: 150–300 mg once weekly Effective in yeasts and less so in dermatophytes.
Secondary prophylaxis Antifungal cream, lotion, or powder daily. Antiseptic gels: ethanol or isopropyl alcohol. Pedicures/manicures: make sure instruments are sterilized or individuals have their own.
spontaneously. Therefore, the incidence increases with advancing age. ETIOLOGIC AGENTS About two-thirds of onychomycosis caused by dermatophytes (T. rubrum most common, T. mentagrophytes). NONDERMATOPHYTE MOLDS From soil. Acremonium, Fusarium, and Aspergillus spp. Often more difficult to treat. PREVALENCE Incidence varies in different geographic regions. In the United States and Europe, up to 10% of adult population affected (related to occlusive footwear).
LABORATORY EXAMINATIONS
Clinical diagnoses of onychomycosis should be confirmed by laboratory testing (see “Dermatophytoses,” Section 26). Clippings of affected nail plate and subungual hyperkeratotic debris can be assessed
via microscopy (KOH, PAS) or fungal culture, which is less sensitive but can identify the causative organism. For proximal subungual onychomycosis, the specimen can be obtained by punch biopsy, if KOH wet mount is negative. After negative KOH wet mounts. PAS stain is used to detect fungal elements in the nail.
COURSE AND PROGNOSIS
Without effective therapy, onychomycosis does not resolve spontaneously, and usually instead progresses to involve other nails.
MANAGEMENT
See Section 26 and Table 32-1. Photodynamic therapy and laser therapy such as long pulse, short pulse, and also Q-switched have also been used recently, though efficacy has been a source of controversy.

FIGURE 32-19 • Onychomycosis of toenails: Distal and lateral subungual type (DLSO) The toenails are white, caused by onycholysis and subungual hyperkeratosis. The dorsum of the feet shows erythema and scaling, i.e., tinea pedis. T. rubrum was detected on culture.

FIGURE 32-20 • Superficial white onychomycosis (SWO) The dorsal nail plate is chalky white. KOH preparation of the curetted area shows hyphae.

FIGURE 32-21 • Proximal subungual onychomycosis type (PSO) The proximal nail plate is a chalky white color caused by invasion from the undersurface of the nail matrix. The patient had advanced HIV/AIDS disease.
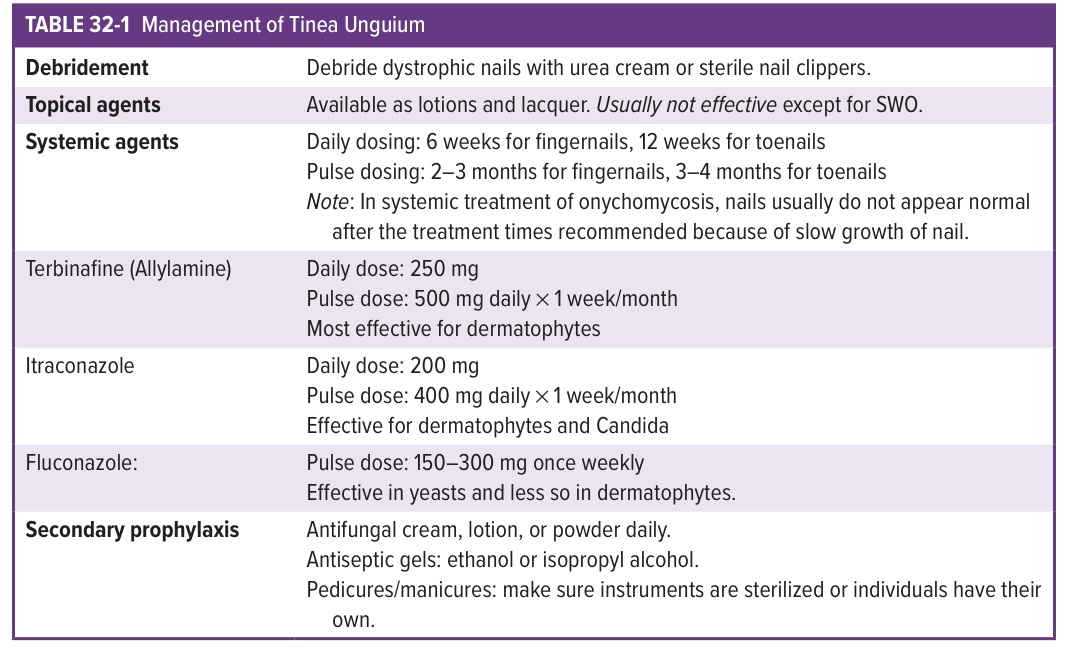
TABLE 32-1 Management of Tinea Unguium